[edit]
Balancing the Risks of Pupils Returning to Schools
This paper has drawn on evidence available up to 10 July 2020. Further evidence on this topic is constantly published and DELVE will continue to develop this report as it is prepared for publication. This independent overview of the science has been provided in good faith by subject experts. DELVE and the Royal Society accept no legal liability for decisions made based on this evidence.
Summary
As we move into a phase of continuously reviewing decisions to keep schools open or shut, we need to recognise there are risks from having schools open and risks from having schools shut. In open schools, the risks to pupils themselves from COVID-19 are very low, though there are risks to school staff, parents/carers and the wider community.
Closing schools causes loss of learning and deterioration in children’s mental and physical health, for example. Keeping schools shut increases inequalities, in both children’s education achievement and their long-term prospects. The goal of “levelling up” therefore needs schools to be open. Keeping schools open is also the key to unlocking the rest of the economy, allowing parents to leave teaching to teachers and return to their own jobs. The evidence on the infection risk from school opening is limited, though to date it suggests that the risk from opening schools, relative to restarting many other activities, is not as high. The experience of most other countries which have already taken this step supports this. By contrast, the evidence on the negative impact of closing schools is considerable and robust.
The report sets out this case in detail. The aim is to provide an evidence framework for understanding the risks involved in re-opening and re-closing schools.
The key issues are the effect of schools closing and re-opening on:
-
risks from infection
-
risks from loss of skills and increases in inequality
-
risks to child and parent mental health
-
risks from parents not being able to return to work.
The report addresses each these in turn, describing first the current state of knowledge, and second, the steps that we can take to collect more data specific to the UK to inform future decisions.
Citation
(2020), Balancing the Risks of Pupils Returning to Schools. DELVE Report No. 4. Published 24 July 2020. Available from https://rs-delve.github.io/reports/2020/07/24/balancing-the-risk-of-pupils-returning-to-schools.html [pdf].
Table of Contents
- Recommendations
- Context
- Schools and infection
- Schools and learning loss
- Schools and health
- Schools and parental employment and earnings
- Commentary on the Government’s school opening plan
- Next steps
- Report Findings
- Technical Appendices
- Appendix: Estimates of the socio-economic gaps in learning
- Footnotes and References
Recommendations
A. Keeping schools open should be the default policy. The Government should do everything feasible in order to not close schools. This means:
-
Suppressing the virus in the wider community to reduce the risk of transmission in schools once at full capacity, and to minimise future disruptions to learning; if local outbreaks occur, other facilities where the risk of transmission is high (such as pubs or gyms) and non-essential shops should be closed, before considering school closures;
-
Providing realistic guidance and substantial extra resources to ensure schools can minimise chains of transmission. This includes: parental guidance, translated into multiple languages, on when to keep their child at home applying the precautionary principle; rigorous hygiene rules; distancing and reduced mixing; extra teachers, PPE (one or two full PPE sets and provision of cloth face coverings for teachers, older children and those with underlying heath issues); management of staff rooms, regular testing and prioritisation for vaccines for teachers;
-
Implementing an effective monitoring regime that can cope with the likely case load in winter, including broad surveillance, linked to an effective, sufficiently scaled and rapid test-trace-isolate system, as well as systematic outbreak investigation. This is all essential to ensure that schools are re-opened as quickly as possible.
B. If local full or partial closures must occur, this should be based on clear scenarios with objective criteria:
-
There must be a set of clear, comprehensible, data-driven and public criteria defining each escalation; these could be presented in the form of a series of pre-defined local alert levels, and will depend on key parameters, such as the number of local cases;
-
There must be associated plans for each escalation. These need to be defined but might look like this:
-
Sporadic cases or clusters in the local community: provide alerts to local schools and families, test, trace and isolate, and where appropriate group isolation.
-
Sporadic cases in school: provide alerts, test, trace and isolate and group isolation (e.g. class/year);
-
Clear clusters in school across year groups: provide alerts, consider individual school closure with outbreak control response to minimise onward transmission and re-open school as quickly as possible;
-
Widespread local community transmission: local area lockdown;
-
Last resort: national scale closures.
-
-
There must be clear responsibility for decision making regarding the closing and re-opening of schools. The key agencies are numerous, including the schools themselves, Local Authorities and embedded public health teams with responsibility for infection prevention and control, Public Health England (PHE) and local Health Protection Teams, the Joint Biosecurity Centre and the Department for Education (DfE). The scope for slow and muddled decision-making is obvious. Before September, these agencies need to determine a coherent chain of command and responsibility to take effective local decisions. While PHE and DfE have set out basic, and separate, criteria for school closure, we are clear that a much more joined up and granular approach is necessary.
C. The Government should urgently initiate data collection:
-
A system, including surveillance studies, must be in place to provide decision-makers with the local and timely data they need to monitor neighbourhood and school infection rates and to respond accordingly. That is, the information structure we set out in A.3 must be integrated with the decision structure in B.3. For example, the minimal data collection from individuals being tested for Covid-19 needs to include whether the person being tested is connected with a school (as teacher or parent), and if so, which school. This information needs to be collated and made available to the relevant decision makers charged with monitoring the conditions for school closures;
-
There needs to be a programme of anonymous assessment of education achievement and pupil mental health across all age ranges in a sample of schools in mid-September, to gauge the extent and nature of the learning loss and impacts on student mental health. Tests should also be administered at the end of the 2020/21 academic year in this sample of schools, to assess any improvement during the year;
-
Given the weak evidence base on both the effectiveness of specific strategies in schools to reduce infection risk, as well as the adaptions that will be needed to mitigate learning and other losses from school closures, we need to encourage experimentation, better evaluation and good knowledge exchange mechanisms to share learning across the education system.
-
We further recommend a cost-benefit analysis of widening the eligibility for influenza vaccination to secondary-school children (or certain age-groups thereof).
D. The Government must establish effective, clear and unified communication with school leaders, teachers and parents to manage opening and closing of schools in response to local conditions. The communication from government to parents should be informed by behavioural science to make sure the messages are salient, clear and consistent.
Context
School closure affects many outcomes, and these are quantified in different metrics. Weighing these against each other to reach an overall decision is crucial. As in other aspects of the COVID-19 response, this can be expressed as “lives versus livelihoods”. This is true for schools also: lives saved by closing schools, set against the lost skills, lower future earnings, and consequent greater poverty. We cannot resolve that trade-off here but given the need to design policies that do the least harm, it is essential that we balance any increased risk to life from schools being open with lives shortened and diminished from greater poverty due to school closures. Our assessment of the evidence suggests that keeping schools open should be the default position given the substantial risks from closures.
While there are many factors to consider when weighing the risks from closing and opening schools, the core issue is the interplay between two dynamic processes: infection and learning. Closing or re-opening schools changes the evolution of both. For infections, school closures may reduce the effective reproduction number. When the infection rate is high, this might potentially result in a large reduction in the number of cases, but when infection rates are low, the reduction in the number of cases may not justify the costs of school closure. The learning process is characterised by dynamic complementarity, meaning that “learning builds on learning”. Missing some school reduces the child’s ability to learn the following material. This means that the gap of lost learning grows at an increasing rate as more and more time is missed from shut schools. The relative benefits and costs of opening or closing schools thus depends upon how long schools have been shut, and the local infection rate.
There are no perfect data to address any of these questions. Much of the discussion below is based on imperfect and incomplete evidence, though it should be noted that the evidence on the learning and other losses from school closures is more robust than that for the impact of schools on infection rates. This means that some of our recommendations are cautious and cannot be expressed with as high a level of specificity as we would normally prefer. Some of our key recommendations are therefore specific ways in which more data can be collected to better inform future re-opening and re-closing decisions.
Schools and infection
1. What happened to infections in other comparable countries when they re-opened schools?
We are able to learn from the experiences of other countries, comparable to the UK, and track the impact on infection rates of opening schools. Comparable international data are shown in Figure 1, before and after school opening. This suggests that, in general, the opening up of schools has not resulted in notable rises in infection at a national level. In all the countries reviewed there have been individual school closures associated with COVID-19 infections in schools, except for in New Zealand.
We note a number of caveats in interpreting the data. First, in most countries other interventions were made at the same time, so that any trends we see may result from a combination of different actions. Second, in some countries the school opening date was recent and it may be too soon to see any effect in the data. Third, in most countries, schools partially opened and a complete return of all pupils may look different.
2. What protective measures did other comparable countries take in schools, and did they help?
As governments around the world introduced phased opening of schools, several risk mitigation interventions (e.g. enhanced hygiene measures, limited interactions, distancing measures, targeted communication strategies and the use of personal protective equipment) were employed to reduce transmission of the virus among pupils and staff.
The type and severity of interventions used vary greatly between countries. Additionally, it is impossible to assess the impact of individual mitigation measures because a combination of procedures was introduced in all settings, and school-level data on interventions and outcomes is not available.
Most countries employed physical distancing measures in schools until cases in the community had been suppressed to manageable numbers. In a few countries, at the time of this writing, distancing measures have been lifted to allow schools to operate at close to normal capacity, e.g. in New Zealand, Australia, France, Switzerland and it is critical that these countries be closely monitored. Furthermore, evidence on transmission of the virus in school settings and the link between school attendance rates and the number of new cases of COVID-19 in the UK should be examined. All these data sets will give us better insight into infection risk in the school setting.
Additionally, enhanced hygiene measures continue to be implemented in most countries, although in countries like New Zealand, this has been greatly relaxed due to successful suppression of the virus. It is recommended that explicit guidance and additional resources are provided to local authorities and schools to ensure that the highest level of hygiene is in place in schools until the winter season has passed, when it can then be reassessed. Consistency should enable these practices to become normative.
There is evidence from other settings on the use of masks. If physical distancing in schools is not possible, masks will play a role in preventing infection. Given the potentially lower infection risk from young children, the difficulty of getting young children to wear masks, and the likely negative impact of masks on their verbal comprehension and language development, the case for primary school children wearing masks is not clear. However, older children, all adults in schools, as well as parents bringing their children into schools, should wear masks. Masks should also be worn on public transport on the way to school in line with national guidance.
Given the limited evidence on the effectiveness of specific mitigations, schools need to try to minimise infection risk using a variety of methods and need to be resourced accordingly.
3. What is the evidence on the level of risk to children, the prevalence of infection among children, and estimates of the level of transmission in schools between children / from children to adults?
The risks to pupils themselves from Covid-19 infection are very low, with life-threatening complications for children being very rare indeed. However, there are risks to school staff, parents/carers and the wider community. The risks to teachers, parents and carers will vary depending on age and underlying health conditions, with some (e.g. grandparent carers) at higher risk than others. Those at higher risk will need to follow the national guidance in this respect.
Whilst early reports suggested that children were much less susceptible to infection than adults, the largest-scale sero-surveillance studies in Europe have so far found only somewhat lower infection-rates in children, versus adults: viz, infection-rates for children of between 60% and 80% of those in adults (and smaller differences were found in countries such as Sweden, where schools for under-16s remained open). The Office for National Statistics (ONS) Infection Survey pilot did not find significant differences in infection-rates in England, between different age-groups, but its current estimates on Nucleic Aciden Amplification Test (NAAT)-positivity-rates in the age-groups 2-9 and 10-19 are based on just eighteen NAAT-positive cases. The evidence-base on the likelihood of adults infecting children is limited, but between them, the highest-quality studies suggest that adults may be approximately half as likely to transmit infection to children in the same household, as they are to transmit infection to adults in the same household. There is also weak evidence that children are less likely than adults to transmit infection to others.
So far, there are very few data-sets available on school-specific transmission, but the balance of evidence so far suggests that schools play only a limited role in overall transmission. This is in marked contrast with influenza, where there is strong evidence that schools are an important driver of overall nationwide transmission. The international data that are available shows at most very limited transmission in schools where a child was the index case.
There is an important need for targeted data-collection, to determine more accurately the frequency of transmission from children to adults and from children to other children (both within schools, and outside), and to determine more accurately the frequency of transmission from staff to pupils in schools. We recommend that any outbreak in a UK school should be followed up by a thorough outbreak investigation, utilising contact-tracing and NAAT-testing of schoolchildren, school staff and household contacts of both. Phylogenetic analysis should be used where appropriate, to investigate probable chains of transmission.
4. Are there significant additional risks for BAME families?
The risk to BAME children, as for other children, is very low indeed. BAME adults are at higher risk from COVID-19 than other ethnic groups. The extent of the additional risk for BAME groups varies by age and pre-existing health conditions. The reasons for the additional risk are fivefold: they are more likely to work in occupations with higher exposure, to have worse living conditions, to suffer from co-morbidities, to access poorer health care and to face discrimination.
Hence some BAME parents, carers and school staff will indeed be at greater risk due to some of these causal factors and need to follow national guidance in respect of their particular risk factors. BAME teachers who do not have these underlying risk factors are likely to be less at risk than the average BAME adult. This is because they do not have a major risk factor faced by many BAME people, which is being in a low-income job.
5. How can we best improve our understanding of schools and infection for the UK?
The key infection question to be answered is whether re-opening schools raises the local infection rate. The international evidence (see 1 above) is cautiously optimistic, but we need data precisely tailored to the UK situation, including data on the prevalence of infection in schools, and on transmission within schools.
To answer this question, we need to assess the outcome from opening schools relative to a counterfactual: what would have happened to local infection rates if schools had remained closed? To do this requires testing of pupils not returning to school, as well as those who do. June and July 2020 offered that opportunity, and we hope that similar circumstances deriving from administrative/institutional decisions will do so also in September.
The COVID-19 Surveillance in KIDs (sKID) programme run by PHE, is a proof-of-concept study that aims to test staff and students in 100 schools this summer mini-half term. An analysis of the sKID data collection protocol suggests that it will not be able to conclusively demonstrate a difference in risk for attending school, even if the risk is double that of non-attendance. This is because the sample size is too low given the current COVID-19 prevalence in the UK, and because sKID plans to test only children attending school. A case-control study of children both in and not in school would allow us to compare how attending school affects the infection rate in children whilst taking into account variation in school facilitates, rates of contact between children outside of school, and regional infection rates.
Surveillance studies such as sKID do require huge sample sizes to be effective when infection rates are low, and so responsive testing and detailed case study analysis of test results (including of phylogenetic data) from schools which have experienced an infection, may be a more feasible approach to understanding transmission in schools.
Schools and learning loss
6. How much learning has been lost, and what is the impact on skill levels from closed schools?
For most pupils in the UK, around 12 weeks of face-to-face learning has been lost, about a third of a year. This is likely to have a very significant impact, greater for younger children, given evidence that investments in children’s learning tend to be complementary over time.
The key methodological challenge is that estimating a causal impact of school time on skills requires a setting with exogenous variation in the former. Consequently, the most robust evidence covers the effects of school closures because of teacher strikes, weather extremes, and other quasi-random settings.
The most robust studies suggest an impact of between 6%SD to 10%SD, for the learning loss. This is roughly equivalent to the difference between being taught by a highly effective teacher for half the year and an ineffective teacher for half the year, compared to being taught by an ineffective teacher all year.
Some of this will have been offset by learning at home and the provision of remote schooling, but this has only been partially effective for most families. Wide variation in the quantity and quality of remote schooling and home learning support between pupils and schools underlies much of the variation in learning loss over this period.
7. Why and how much does learning loss matter?
The evidence shows that schooling raises skills, and so while qualifications are in part simply a “signal” of ability, missed school means lower skills which have real implications for individual lives and for the economy as a whole.
First, a huge base of evidence shows that earnings depend on skills, and lower skills means lower earnings. For example, if a student misses a third of a school year, and each school year brings roughly a 10% return, earnings potential is likely to be permanently lower by around 3% a year. Students at the lower end of the ability distribution are more likely to have lost heavily from school closure and are more likely to be low earners, so will face a significantly higher risk of poverty. Evidence from the prevalence of teacher strikes in Argentina shows that exposure to average strike incidence in primary school reduces earnings in mid-life for women by 1.9% and for men by 3.2%.
At the national level, lower aggregate skills will reduce the growth rate. The magnitudes are not trivial: 13 cohorts of students have been affected by the lockdown, so from the mid-2030s for the 50 years following that, around a quarter of the entire workforce will have lower skills, with a consequently lower growth rate. The present value of such a fall in the growth rate is measured in billions not millions. For example, the study of teacher strikes in Argentina estimates the aggregate earnings loss in Argentina from lower skills of $2.34 billion per year.
One of the consequences of lost skills from closed schools is greater risk of poverty: earlier research from the ONS shows that “those with a low level of educational attainment are almost five times as likely to be in poverty now as those with a high level of education”. There is a huge literature linking poverty to ill health and early death, though isolating a causal relationship is always difficult. One example shows a 7.9 year gap in life expectancy for women and a 9.7 year gap for men between the most and least deprived deciles of areas poverty.
8. What is the likely impact on inequality?
The actual loss of learning in the current pandemic will vary by context, depending in part on what schools and families have been able to provide in the way of remote schooling. It is very likely that these gaps in provision have exacerbated existing inequalities between students from low and high socio-economic status families.
Our analysis of new achievement data from an online learning platform in the UK shows significant increases in the test score gap between high and low performers pre- and post-school closure.
The Education Endowment Foundation presents a meta-analysis of the existing literature. They calculated that school closures will widen the attainment gap between poor and non-poor families. Their meta-analysis suggests a median impact of 36% (the range of this estimate is between 11% and 75%) by September 2020.
Differences in parent/carer knowledge and ability to help their children, differences in parent/carer time available, differences in availability of quiet study space in the home, differences in the availability of IT kit and fast internet, and the differences in the provision of useful material by the school are all correlated with family income and contribute to growing inequality. This is supported by a number of high-quality studies undertaken since the beginning of remote schooling.
From a school perspective, a survey of teachers and Headteachers by NFER reinforced this view. Most teachers were covering less of the curriculum than normal, and pupils were doing much less work than normal. Teachers reported that pupils from poor families were less engaged with their work. Three-quarters of senior school leaders reported that their schools were offering ‘social or welfare’ support to vulnerable pupils, and half reported significant concerns for the safety and wellbeing of vulnerable pupils.
9. Specifically, what has happened to BAME children?
Higher levels of educational attainment are correlated with higher family income and higher parental education. Since BAME pupils on average come from households with lower levels of income, this in turn impacts on their education level. According to the ONS, children in Bangladeshi and Pakistani households were most likely to live in low income and deprived areas out of all ethnic groups. The relationship between deprivation and education is the key to understanding life chances. Children of these ethnic groups with lower levels of income are more likely to have been significantly badly affected by school closures.
GCSE scores shows wide variation within the BAME category. Students of Asian ethnicity, including but not only Indian and Chinese students, as well as Black African students, score above White British students, while Black Caribbean students are about level with White British ones.
There is also evidence to suggest a more positive attitude to learning and to school in general among some BAME students, particularly those who are the children of immigrants. This higher level of existing achievement plus more positive attitudes may to a degree help to offset the effect of higher poverty levels on the impact of school closures.
10. How can we best improve our understanding of learning loss in the UK?
We do not currently have direct measures of children’s learning loss as a result of the school closures. This is clearly a major data gap. The first step is therefore to collect the necessary test score information needed to estimate the scale of the learning loss from school lockdown.
Ideal study designs to properly gauge the learning loss from lockdown are not available. Almost all pupils were undertaking remote schooling, so there is no natural control group; and a simple longitudinal approach is not possible because very few schools are testing pupils as this report is written (early July 2020).
The first date of general testing will be the return to school in September. Because there is no national, officially sanctioned test for all age groups at that date in the UK, we recommend an additional test at the beginning of the academic year and one at the end (the latter to assess improvements during the year). The burden on schools now and more so in September will be large, so we also recommend that these tests be carried out on an anonymous sample of schools, rather than be universal.
For these tests to have any value, there has to be a comparator with the previous cohort, a “before” benchmark. Consequently, we recommend using tests that have a ‘synthetic’ before score – that is, normed tests that have a known and validated typical score in normal times.
The age-appropriate tests would be taken by pupils of all age groups in school in September 2020 in samples of schools; ideally, we would pick different schools per age group to sample a wider range of school effects, with some useful regional spread. The follow up test would be administered at the end of the academic year 2020/21. The exact sample size required depends on the test used but in broad terms it is estimated that around 150 schools per secondary school age group and around 600 schools per primary school age group would be required.
Schools and health
11. What are the other losses for the children from closed schools?
Evidence from the impact of school holidays suggests that children may be less active and have worse diets as a result of being out of school.
Previous research also suggests that being out of school and more isolated will impact negatively on children’s mental health. The impact is likely to be greater for children and young people with pre-existing mental health conditions and in more socio-economically deprived households. Social isolation and lack of contact with peers is likely to be particularly harmful for adolescents.
Evidence from the pandemic on the impact on children’s mental health is still relatively limited and of variable quality. However, it does suggest adolescents are particularly negatively affected, as are vulnerable children, those with particular conditions (e.g. autism) and children in care. This will have been exacerbated by more limited access to public services, particularly mental health services.
Establishing the causal impact of shutting and closing schools on children and young people’s health is challenging methodologically since lockdown has involved a range of other social restrictions. Proposals made in this report to measure the impact of school closures on learning loss (see 10 above) should be extended to measure the impact on child and adolescent mental health and wellbeing using the same methodology.
Schools and parental employment and earnings
12. What are the other losses for parents from closed schools?
In terms of wider impacts, it is clear that children being schooled at home has had a negative impact on parents’ ability to work, particularly women. This impact is well documented, though the long-term impact of these changes is unclear. What is clear is that the ending of the furlough scheme will significantly sharpen the need for many families to return their children to school so that they may return to their jobs. If schools return in September and no further lockdowns occur, it is conceivable that the impact of school closures on parents’ earnings and career trajectories will be limited (though clearly there will be an impact from any downturn in the economy). If, by contrast, schools do not return full time or we have repeated lockdowns, the impact on parents’, and particularly women’s, labour market trajectories is likely to be major.
This in turn affects household income and the greater burdens falling on low-income families will widen income inequality. It also adversely affects gender equality in the workplace and in the home. For low-income families, the loss of income and the degradation of future prospects may push them in to poverty (noting that one in five children already live in poverty). Currently around one in five parents in low income occupations have children and cannot work at home. This group will be particularly at risk of job losses if schools do not stay open.
13. How can we best improve our understanding of these other losses?
Open access data sets are coming on stream that can help us monitor the impact of the lockdown on children and young people’s physical and mental health, and indeed the employment circumstances of parents. Longitudinal follow ups are vital if we are to accumulate sufficient evidence on the impact of lockdown on children and young people’s health, as well as parental employment and household economic circumstances.
Commentary on the Government’s school opening plan
We note the recent (2/7/20) Department for Education (DfE) guidance regarding school opening in September 20201. Its recognition of the significant costs of school closures, as well as the need to minimise the risks from opening schools, is to be welcomed. Our report supports the DfE position that all children need to return to face to face schooling wherever possible and that keeping schools open should be prioritised. School attendance must indeed be compulsory for the majority of children (i.e. those who are not at particular risk from COVID-19) and decisions to open and shut schools must be made on objective criteria with closures minimised. As we state above, what is urgently needed are clear and well communicated criteria to guide school closures and re-openings. This will also help to address teacher, parent and carer concerns about pupils returning to school.
The DfE guidance provides a lot of specific information for schools on how they should open and operate, as well as what will be required in preparation for a potential return to remote teaching during any future school closures. No doubt this guidance will change as the situation changes and more evidence emerges as to the effectiveness of different strategies to minimise infection transmission. Clear, realistic and timely communication with school leaders and teachers is vital. It is a major challenge to change ways of working in schools, particularly in a fast-moving environment with rapidly changing guidance. This needs to be recognised and guidance kept as simple and stable as possible. Further, some of the changes that are required of schools will need additional resource (whether that be in terms of additional staffing or pieces of PPE and other kit). This too needs to be recognised and an adequate level of resource provided. The challenge of simultaneously adapting schools to the safety mitigation procedures required, alongside also ensuring that adequate provision will be available in the event of subsequent school closures, should not be underestimated. The DfE guidance also proposes additional resource to support academic catch up for pupils who have fallen behind. This will be vitally important if we are to mitigate some of the increasing inequality in academic achievement that we are likely to see as a result of the pandemic. The DfE guidance that schools need to support children’s wellbeing when they return is also supported by our report. However, again additional resources will be required. We also recommend that the Government develops policies and provides additional resource to support those students who have experienced learning and other losses from school closures to ensure they are not disadvantaged over their lifetime. We need to mitigate the economic scarring that will result from educational deficits in particular. The Government also needs to consider long term options to support re-entry to educational opportunity later in life for those disadvantaged by COVID-19 now.
Next steps
There is much we still do not know. Further surveillance and studies are needed to:
-
Determine the extent to which children of different ages transmit COVID-19, including undertaking school case studies to better understand transmission processes;
-
Understand the effectiveness of different interventions and strategies designed to reduce infection transmission in schools, including learning from strategies being adopted in other countries;
-
Measure the learning and other losses from school closures during the pandemic; identify successful school interventions to reverse the detrimental impact of school closures on learning loss and other outcomes;
-
To address (2) and (3) we need to encourage experimentation, better evaluation, and good knowledge exchange mechanisms to share learning across the education system.
Report Findings
1. Background
As we move into a phase of continuously reviewing decisions to keep schools open or shut, we need to recognise there are risks from having schools open and risks from having schools shut. In open schools, the risks to pupils themselves from Covid-19 are very low, though there are risks to school staff, parents and the wider community. Closing schools causes loss of learning and deterioration in children’s mental and physical health, for example2. Keeping schools shut increases inequalities, in both children’s education achievement and their long-term prospects. The goal of “levelling up” therefore needs schools to be open. Keeping schools open is also the key to unlocking the rest of the economy, allowing parents to leave teaching to teachers and return to their own jobs. The evidence on the infection risk from school opening is limited, though to date it suggests that the risk from opening schools, relative to restarting many other activities, is not as high. The experience of most other countries which have already taken this step supports this. By contrast, the evidence on the negative impact of closing schools is considerable and robust.
The report sets out this case in detail. The aim is to provide an evidence framework for understanding the risks involved in re-opening and re-closing schools. The key issues are the effect of schools closing and re-opening on:
-
risks from infection
-
risks from loss of skills and increases in inequality
-
risks to child and parent mental health
-
risks from parents not being able to return to work.
The report addresses each of these in turn, describing first the current state of knowledge, and second, the steps that we can take to collect more data specific to the UK. The aims of this report are therefore two-fold. The first is to summarise existing evidence, including pre COVID-19 evidence, that can help us understand the likely risks of school opening/closing on infection rates, children’s learning and other outcomes being affected by the closure of schools. In the absence of better data, this can help inform policy decisions. As noted above the quality of the evidence available does vary enormously, depending on the specific issue being considered. We have not been able to undertake systematic reviews of the existing literature and we do our best to guide the reader as to the nature of the evidence and its robustness. The second aim is to document the data that we do have on the impact of this crisis in relation to schools and to articulate the kinds of data collection that are needed to plug gaps in our understanding. There are of course a number of important issues related to education that we have not been able to consider in this report. For instance, we need to ensure that those left behind now in terms of their education achievement are not disadvantaged forever, and to mitigate the sizeable economic scarring that will arise from educational deficits. The Government has already announced some strategies in this respect, more will be needed. In the longer term it will also need to consider options to support re-entry to educational opportunity later in life for those disadvantaged by COVID-19 now. These important long-term term issues merit further consideration but are not discussed here.
In the UK schools moved to remote teaching and learning in March, except for key worker children who were permitted to attend in person. Remote schooling provision has been highly variable in terms of quality, with some students struggling to access support. Further, remote schooling cannot easily substitute for the social contact with other adults and peers that children also get from attending school in person. Despite the best endeavours of schools, the consequences of children having minimal or poor quality schooling for such an extended period of time is likely to be that they miss out on a substantial amount of learning, have poorer health (particularly mental health) and for some children it will potentially put them at greater risk of neglect or abuse. Additionally, the toll on some parents from trying to home school their children is likely to be substantial, both in terms of parents’ wellbeing and their ability to do their paid work. If children receive remote schooling on this basis for an even more extended period of time, these negative impacts will be greater and longer lasting.
In England, some year groups have already returned (or will be returning) to school during the 2020 summer term. The Government has also stressed that schools will be open for all children in September 2020, though policies may vary across the countries of the U.K. However, it is likely that ongoing decisions will need to be made about closing and reopening schools during the academic year, depending on the prevalence of the virus. Decisions about schools opening, and indeed closing again in the event of infection spikes or a second wave, must be firmly guided by the relative risks of different courses of action. First, the risk to public health in terms of transmissions and the need to maintain an effective reproduction number (Re) below 1. Equally such decisions must also involve consideration of the risks of closure on learning loss and children’s future life chances, as well as risks for parents’ jobs and earnings.
While there are many factors to consider, the core issue is the interplay between two dynamic processes: infection and learning. Closing or re-opening schools changes the evolution of both. For infections, school closures may reduce the effective reproduction number. When the infection rate is high, this might potentially result in a large reduction in the number of cases, but when infection rates are low, the reduction in the number of cases may not justify the risks and costs of school closure. The learning process is characterised by dynamic complementarity, meaning that “learning builds on learning”. Missing some school reduces the child’s ability to learn the following material. This means that the gap of lost learning grows at an increasing rate as more and more time is missed from shut schools. The relative benefits and costs of opening or closing schools thus depends upon how long schools have been shut, and the local infection rate.
To help inform such difficult decisions, it is imperative that analysts have access to good data that can enable robust estimation of the increase in the infection risk from opening schools, as well as the negative impact on children’s learning and other outcomes from closing schools. Currently we have insufficient high-quality data on both these elements, an issue which needs to be urgently addressed. Further, decisions about opening and closing schools are likely to need to be made at a local level, in response to spikes of infection in some localities. Hence there is also a need for effective surveillance mechanisms and for data to be available at the local area level. The UK is also not alone in facing these decisions. Almost every other country also closed their schools. Likewise, most countries are currently drawing up plans to open their schools, and many have indeed opened schools already. We can learn from the experience of other countries and international collaboration and sharing of data is vital. Lastly, another focus of this report is on how schools can open safely with infection mitigations in place. Yet we have very limited robust evidence on the effectiveness of any such mitigations. Prospective studies should try to evaluate not only the infection risks from opening schools but also the impact of different mitigations: again we might learn much from considering what other countries are doing.
2. Opening Schools Safely
In this section, we summarise the guidance provided by intergovernmental organisations on schools during the COVID-19 pandemic, the emerging evidence on transmission of the virus, the approaches adopted by select countries to reopen schools and the data required to allow schools to manage school operations during this pandemic.
a. Intergovernmental Guidance
In March, the World Health Organization (WHO), the United Nations International Children’s Fund (UNICEF) and the International Federation of Red Cross and Red Crescent Societies (IFRC) provided detailed high-level guidance on the prevention and control of COVID-19 in schools3. In this report, a checklist of core non-pharmaceutical interventions (NPIs) such as, enhancing hygiene, improving airflow and providing clear communication on the risks of COVID-19 was provided. In addition, the WHO’s Public Health and Social Measures Annex on schools- published in May4-recommended that governments should adopt a risk-based approach to determine if, when and how schools readmit pupils. It also suggested that decision-makers should be informed on the latest evidence on transmission of SARS-CoV-2 among children and the severity in children, the local situation and epidemiology of COVID-19 where schools are located and the school setting and ability to maintain COVID-19 prevention and control measures. In this guide, a more detailed list of NPIs was provided, including case management, one metre distancing measures, limited class sizes, staggered start and end times, leveraging outdoor space, the use of “tele-schooling” and developing a policy to ensure masks or face coverings are worn in line with national or local guidance3,p.4. In June, UNICEF, the World Bank, the World Food Programme and UNHCR provided a framework to help governments choose the policies that are most suitable locally5. The United Nations Educational, Scientific, and Cultural Organisation (UNESCO), the World Bank and other international groups have also provided additional guidance to Ministries of Education across the globe.
b. Schools and infections
Evidence on COVID-19 prevalence among children, illness severity among children, transmission from adults to children and from children to adults, and transmission in schools.
While there are still gaps in the evidence-base, and better-quality studies are continually emerging, the available evidence (internationally) indicates that we can draw the following conclusions at this time.
There is good evidence that the prevalence of Covid-19 infection among children has generally been either similar to the prevalence among adults, or lower, in the UK and internationally. More data are required to judge whether prevalence in the UK is significantly lower among children than among adults, or whether prevalence is similar among children to among adults. We proceed to outline the evidence.
Firstly, we observe that the ONS Infection Survey pilot6 (for England) has not found a statistically significant difference between rates of NAAT-positivity in children, versus in adults, with nine out of 3,117 children aged 2-11 testing positive (NAAT-positivity rate 0.29%; 95% CI: 0.13% to 0.55%), and nine out of 2,860 individuals aged 12-19 testing positive (NAAT-positivity rate 0.31%; 95% CI: 0.14% to 0.60%), between 26th April and 27th June. These should be compared to NAAT-positivity rates of 0.42% (95% CI: 0.31% to 0.56%) in the age-group 20-49, and 0.28% (95% CI: 0.20% to 0.39%) in the age-group 50-69. However, the confidence intervals for the different age-groups remain wide, due to the low rates of NAAT-positivity. Hence, more data are required for us to judge accurately whether prevalence in England is significantly lower among children than among adults, or whether prevalence is similar. The ONS data do, however, provide good evidence that the rate of NAAT-positivity in children in England, between 26th April and 27th June, was not much higher than that in adults.
We do not yet have reliable age-specific seroprevalence data for England. However, the very large Spanish ENE-COVID seroprevalence survey7 found a statistically significant difference between seroprevalence levels in children versus in adults, with that in children being lower. This was a survey of 61,075 individuals between 27th April and 11th May; one of the highest-quality seroprevalence studies to date, worldwide. From this survey, seroprevalence in children in Spain aged 5-9 was estimated at 3.1% (95% CI: 2.2%-4.2%); in children aged 10-14 at 4.0% (95% CI: 3.1%-5.0%), and for those aged 15-19 at 3.7% (95% CI: 2.9%-4.8%). This compares with an overall population seroprevalence estimate of 5.0% (95% CI: 4.7% to 5.4%), for the Spanish population as a whole. The Spanish lockdown was particularly stringent for children, with under-14s not allowed to leave their homes between 14th March and 25th April; however, it was also stringent for adults - who, with the exception of key workers, were only allowed to leave their homes to buy essential supplies, or in the case of an emergency. Moreover, many COVID-19 infections in Spain will have been contracted before the lockdown was imposed (14th March), i.e. when most schools and workplaces were still open.
There are also relevant prevalence data from Italy. Following the first death from Covid-19 in Italy, in the municipality of Vò, more than 85% of the population of Vò was NAAT-tested in late February, and no positive cases were found among the 217 children aged 10 or under who were tested (NAAT-positivity rate 0.0%; 95% CI: 0.0% to 1.7%), despite 73 out of the 2,812 people tested (NAAT-positivity rate 2.6%; 95% CI: 2.0% to 3.3%), testing NAAT-positive8. Among the 250 individuals aged 11-20 who were tested, three tested positive (NAAT-positivity rate 1.2%; 95% CI: 0.25% to 3.5%). The start of the two-week lockdown in Vò coincided with the testing; schools had been open up until that point.
In some countries, most schools were kept open throughout the pandemic. Iceland has kept schools for under-16s open throughout the pandemic, though it closed upper secondary schools (for those aged 16 and above), from 13th March until 4th May. Population screening in Iceland9 in early April found no SARS-CoV-2 NAAT-positive children under 10 years old, out of the 848 tested (NAAT-positivity rate 0.0%; 95% CI: 0.0% to 0.43%), as compared with 100 testing positive out of the 12,232 tested persons of aged 10 or older (NAAT-positivity rate 0.8%; 95% CI: 0.7% to 1.0%). Iceland, however, has had low prevalence across all age-groups.
Sweden has also kept most schools for under-16s open, though high schools (for those aged 16 and above), and universities, were advised to close and switch to distance learning, from 18th March, and local decisions could be taken to close schools for younger children thereafter, in the case of local outbreaks. According to an announcement10 by the Swedish Public Health Agency, a medium-sized (n=1,104) seroprevalence survey in Sweden found that by the end of April, 4.9% of those aged 0-19 tested positive for SARS-CoV-2 antibodies, compared to 6.7% of those aged 20-64. The full results of this survey have yet to be published (even in preprint form).
Overall, we can say that the risk to children arising from Covid-19 infection is low. We can be essentially certain that the risk of death and of severe illness from Covid-19 infection in children is extremely low. Specifically, the infection fatality rate for children aged 5-14 is estimated at 14 per million (95% CI: 6.6 per million to 24 per million)11. This is lower than the infection fatality rate of seasonal influenza among children aged 5-17 during the 2018-19 ‘flu season in the United States, which was estimated by the CDC at 28 per million12, and is substantially lower than the overall population infection fatality rate of Covid-19, which is approximately 13 per thousand for the UK (95% CI: 11 per thousand to 15 per thousand) 13. As of 23rd June, only five COVID-linked deaths of UK children under the age of 18 had been recorded, and we are only aware of one such death in which no pre-existing health condition was known. Severe illness is also much rarer in children than in adults. The percentage of symptomatic cases requiring hospitalisation is estimated14 to be 0.1% among children aged 0-9 and 0.3% among those aged 10-19, compared to an overall population hospitalisation rate of 4.4%, for the UK. A recent SJD (Barcelona) study15, following 724 children living in the household of a confirmed Covid-19 case, found that more than 99% of the children in the study who subsequently tested positive, had only mild symptoms.
An extremely rare but severe Kawasaki-like multisystem inflammatory condition has been linked to SARS-CoV-2 infection in children. When linked to SARS-CoV-2 infection in under-18’s, this condition is known as ‘Paediatric Inflammatory Multisystem Syndrome Temporally associated with SARS-CoV-2’, or PIMS-TS. The Royal College of Paediatrics and Child Health estimated that, by early June, there had been approximately 200 cases of PIMS-TS in the UK among under-18’s16. The most comprehensive UK study of this syndrome to date (of which we are aware) is that of Davies et al17. This was a multicentre observational study of all children admitted to 19 participating Paediatric Intensive Care Units (PICUs) in the UK between 1st April and 10th May, who fulfilled the case-definition of PIMS-TS. There are a total of 23 PICUs in the UK, of which two were closed during the study period, having been converted into ICUs for adults due to Covid-19, so it can be expected that this study covered at least 90% of cases admitted to PICUs in the UK. There were 78 cases admitted to the 19 participating PICUs in this 40-day period; two of these children died. The median age of all these patients was 11 years. Only 22% tested NAAT-positive for SARS-CoV-2; the other 78% tested NAAT-negative; but 24/25 (96%) of NAAT-negative patients who also underwent a serological test, tested IgG serology-positive for SARS-CoV-2, indicating prior infection with SARS-CoV-2. These data represent an ICU-admission rate (for PIMS-TS) of approximately 1.1 children per million, per week, during the 40-day period of the study. While still being an extremely rare event, children of Black and Asian ethnicities were more likely to be affected; for children of black ethnicity, the ICU-admission rate per week was about 6.3 children per million per week, and for children of Asian ethnicity, the rate was 4.3 per million per week. For comparison, in 2018, there were 26 ICU admissions per week per million children, in the UK (all causes).18
In view of the above, we can be essentially certain that Covid-19 infection typically produces milder symptoms in children, than in adults. This means that the risk of severe disease is less in children, but also that children may more often carry the disease without detection. The proportion of children who are truly asymptomatic (as opposed to pre-symptomatic or pauci-symptomatic, at a given time) remains unknown. Data from Italian emergency departments suggested that 21% of SARS-CoV-2 NAAT-positive children were asymptomatic at the time of testing, but there was no follow-up to determine whether these children later developed symptoms; some could therefore have been pre-symptomatic. Other studies have found comparable figures, but we are not aware of any such study where follow-up was performed.
The balance of the available evidence suggests that children may be less susceptible to infection than adults, given the same level of exposure. Four high-quality studies found odds-ratios for secondary attack ratios of children, versus adults of 0.16 (95% CI: 0.06-0.46)19; 0.27 (95% CI: 0.13-0.55)20, 0.21 (95% CI: 0.11-0.41)21 and 0.34 (95% CI: 0.24-0.49)22, though one high-quality study, of Bi et al23, found no significant difference, with an odds-ratio of 0.82 (95% CI: 0.48-1.43). The very high-quality study of Zhang et al,2222 which found an odds-ratio of 0.34, excluded spouses for this purpose, and also considered only primary cases who were quarantined after diagnosis in local government facilities.
The study of Q.-L. Jing et al20 also contained ten primary cases under the age of 20. The overall secondary attack rate for these cases was estimated at only 5.2% for household contacts (95% CI: 2.4% to 9.7%), and at only 1.4% for non-household contacts (95% CI: 0.04% to 7.6%). For primary cases between the ages of 20 and 59 (of whom there were 145 in the study), the corresponding secondary attack rates were 14.8% (95% CI: 11.7% to 18.4%) for household contacts, and 2.2% (95% CI: 1.4% to 3.4%) for non-household contacts. This indicates that children may be less likely than adults to transmit COVID-19 infection, though studies with a larger number of children as primary cases are needed, to be more certain of this conclusion.
So far, there is limited evidence available for quantifying the extent to which schools contribute to overall nationwide transmission of Covid-19, partly as many countries closed schools early on in their epidemics. The balance of evidence available so far suggests that schools play only a limited role in overall transmission24. This is in contrast with influenza, where there is strong evidence that transmission among children in schools is an important driver of overall transmission25,26. We outline some of the evidence below.
One of the most extensive studies for which results are available was a contact-tracing study27 across 15 schools in New South Wales, Australia, from 5th March to 3rd April. This study involved 18 initial cases (nine children and nine teachers) who had opportunities to infect others. It indicated very limited transmission in a school setting, with just two likely secondary cases arising, both being students (one in a primary school, where the likely primary case was a teacher; and one in a high school, where the two likely primary cases were students). In detail, the six initial cases in primary schools (five staff and one pupil, across five schools) were judged to have 168 close contacts between them; of these contacts, 137 were pupils and 31 were staff. Just one additional case was detected, though in some cases, contacts were only tested if they developed COVID-like symptoms, so only 32% (53 out of 168) of contacts were tested (indicating a risk of possible undercounting of asymptomatic secondary cases). In the primary school where the single additional case was found, there was just one initial case (a staff-member). In that school, 21 close contacts of the initial case underwent serological testing; no other additional cases were found. A review found that it was most likely (but not certain) that this additional case (a pupil) was infected in the school environment, i.e. it was likely to be a secondary case corresponding to transmission from the primary case in that school (who, as mentioned above, was a staff-member). The 12 initial cases in high schools (8 students and 4 staff), were judged to have 695 close contacts between them, of whom 598 were students and 12 were staff. Only one additional case was detected (a student). Nose/throat swabs were taken from one third (235 out of 695) of these close contacts, for NAAT-testing; all of these tested negative. In one high school, where there were two initial cases (both students), 75 close contacts underwent antibody testing one month after contact with one (or both) of the two initial cases. Just one of these contacts (a student) tested positive.
During February and March, the nationwide test-trace-isolate programme in Singapore detected (through NAAT-testing of contacts of confirmed cases in the wider community), three index cases of Covid-19 in schools, as described in the study of Yung et al28. One was a pre-school student, aged 5, another a secondary school student, aged 12, and the third was a pre-school teacher. Only the third index case (a teacher) is thought to have caused any secondary cases, and no secondary cases were detected among students. In the first two cases, the students in question were found to be NAAT-positive from contact-tracing following their exposures to adult household-members who were part of a community cluster. Both students attended their respective schools on the first day of their symptoms, before being subsequently diagnosed with Covid-19 and isolated in hospital. No secondary cases were detected in either of these two schools. All close contacts of the index cases (including all classmates) were placed under a 14-day quarantine and requested to monitor their symptoms; those who were not deemed close contacts were permitted to continue with classes, and asked to monitor themselves for possible symptoms; they were admitted for Covid-19 evaluation if they became unwell during the subsequent 14 days. Eight students from the secondary school developed COVID-like symptoms during the 14-day period and were NAAT-tested, but all tested negative. Similarly, 34 student contacts from the pre-school developed COVID-like symptoms during the 14-day period and were NAAT-tested; all tested negative. However, in the preschool setting where the primary case was a teacher, 16 other cases of Covid-19 infection were confirmed among adult staff-members in the preschool, with an additional 11 cases subsequently being discovered in their households. A total of 77 children from this preschool (73% of all students) underwent NAAT-testing; all tested negative. The remaining 27% who chose not to provide a swab, did not develop any symptoms while under close monitoring and quarantine.
Finally, the study of Heavey et al29, of all reported COVID-19 cases in Irish schools from 1st March to 13th March, found six index cases (three students and three teachers), but no secondary cases were detected in school settings, despite 1,155 school contacts of these six index cases being identified. The only detected (probable) secondary case was in an adult, not in a school setting. (We remark that only those contacts displaying any possible symptoms, including mild symptoms, were NAAT-tested, so some asymptomatic secondary cases might have gone undetected.) According to the report, the available epidemiological data for all six index cases indicated that they had not been infected with SARS-CoV-2 in the school setting.
We note that there have been some other studies and media reports concerning COVID-19 outbreaks in schools, for example, at a school in Oise (Northern France)30, at Gymnasia Rehavia middle and high school in Jerusalem (Israel)31, and in a school in Santiago (Chile)32. However, in the schools in Oise and Jerusalem, it is unclear whether the initial cases were pupils or staff; in the school in Santiago there is good evidence that the index-cases were parents or teachers and that transmission took place during a week of parent-teacher evenings; and in the schools in Oise and Santiago there appears to be no evidence that transmission took place within the schools (excepting in the parent-teacher evenings in the school in Santiago). We are not aware of any official outbreak report or academic study on the Gymnasia Rehavia (Jerusalem) middle and high school outbreak.
- Particular risks from infection for BAME families and teachers
Risks from COVID-19 are higher for some groups than others, for example varying by age and underlying health conditions. Clearly, as in other professions, care will be needed when opening schools to consider the health risks, and necessary mitigations, for older teachers and those who have been sheltering with particular underlying health conditions. A key question when opening schools is also whether teachers and parents from BAME groups33 may be at particular risk and hence whether this should be taken into consideration when making decisions about school opening/closing.
The issues Black, Asian, and Minority ethnic groups are facing in the U.K. mirror those seen among minorities in the United States. According to the latest Public Health England report, Black, Asian, and Minority Ethnic populations have been disproportionately impacted by COVID-19. Five possible factors contribute to the increased vulnerability of members of the BAME community: Occupation, Living Conditions, Comorbidities, Healthcare Bias/accessibility, and Discrimination.
BAME families are overrepresented in low wage jobs and overcrowded areas, making them more vulnerable to COVID-19. BAME households are often extended and multigenerational cohabiting families34. In England, Black people are nearly four times as likely as white people to have no access to outdoor space35. Higher proportions of BAME people live in deprived areas of London and more likely to have concerns over safety and security. Due to these living conditions, when one member of the family contracts COVID-19, is it highly likely the rest of the family will contract the virus. The most deprived areas of England and Wales had more than double the number of COVID-19 related deaths than the least deprived areas (58 deaths per 100,000)36.
Studies have linked comorbidities to poorer COVID-19 outcomes, specifically hypertension, and diabetes37,38. Previous studies have shown that Black and South Asian populations in the U.K. have three to five times the prevalence of type-two diabetes compared to the white people and are diagnosed at a younger age39. Comorbidities are not only a risk for BAME adults but also children from BAME backgrounds. In a small London U.K. study by Harman et al., 80 percent of children admitted to the hospital were from BAME backgrounds with comorbidities40. Studies in the United States and Canada showed that 80 percent of the children admitted to pediatric intensive care units had underlying chronic diseases: immune suppression, obesity, diabetes, seizures, or chronic lung disease41. Teachers and children from BAME backgrounds who have pre-existing conditions should certainly be risk assessed before returning to school settings.
Historically racial and ethnic minority patients have reported unequal treatment by physicians42. When they go to the doctor, they are less likely to receive medication for the same injuries as their white counterparts43,44. Some BAME individuals may also be disadvantaged if medical advice is not translated into the relevant language, an issue that is clearly very relevant during this pandemic during which advice has been complex and changing. People from BAME backgrounds have also reported that doctors are less likely to take their complaints seriously. Systematic racism has created the conditions for minorities to be positioned to be disproportionately affected by COVID-19. Black and Minority Ethnic persons are regulated to poor neighbourhoods and low wage risky jobs, leaving them more exposed to the virus. Black people are more likely to be unemployed, suspended from school, and searched by the police45. Not only does racism create disadvantaged positions, but it also increases their risk of hypertension and diabetes. David Williams’ Everyday Discrimination scale shows that people who experience racism and discrimination have a higher risk of hypertension and diabetes due to high levels of stress hormones remaining in the body for an extended period46.
c. International evidence on schools reopening
The risks from school opening depend of course on the mitigations to reduce infection that schools put in place. This is new territory for schools and there is a critical need to understand from other countries how schools can open safely at close to full attendance. Robust evidence on effective mitigations is however, limited.
Although, approximately 107 countries had implemented temporary school closures by 18th March 2020, multiple countries around the world have opened schools for face-to-face teaching with varying control measures47. A review of the approaches used by countries which are at more advanced stages of the outbreak or who have lower cases of COVID-19 may offer lessons for the UK. In this summary, the school policies used in seven countries were analysed: Germany, France, Spain, Italy, Denmark, Israel, New Zealand, and Australia (see Addendum TD1 for detailed country profiles). Other countries that used notably different interventions are also noted.
The education response has been relatively haphazard in a number of countries, including in high-income countries who are not used to contingency planning or intersectoral planning and response. This has resulted in some confusion for schools, parents and children, resulting in changed plans at short notice, e.g. when schools would operate at full capacity in Germany, France, Spain and the UK. Certainly, there is still a need for clear guidance on how to open schools more safely and summaries of best practices have been developed48. It is also evident that over the course of the outbreak, as evidence was generated, countries have adopted largely similar approaches to reopening.
Governments across the globe were keen to open up schools as quickly as possible to ensure minimal loss of, learning, reduce indirect health harms and ensure that parents could re-join the workforce. However, shutdown periods that involved no teaching – virtual or in-person - varied greatly in time across the globe. Some countries only closed schools for three weeks, e.g. Denmark, while others were shut for seven weeks or more, e.g. in Italy and Spain. Although a few countries controversially kept schools physically open throughout the outbreak, e.g. Sweden and Australia, local governments, local authorities, or school boards implemented closures to varying extents to allow for physical distancing measures.
All countries reviewed in this summary have implemented a phased return to in-person teaching, including in Australia and Sweden (see Table 1, Technical Document 1). In most countries, the children of key workers and the youngest children requiring most supervision were able to return to school before their peers. In Israel and France children with disabilities were also the first to return to schools. The decision to prioritise younger pupils – because as discussed in section 3 the early years are fundamental to reducing educational inequalities and to allow parents to return to work – is a political and economic one. A few countries also prioritised the return of the oldest children who were taking official exams, e.g. in Germany and Israel.
Many of these countries are still operating at partial capacity, leveraging rotating schedules to allow for distancing measures to be employed in schools, e.g. in Germany, Denmark, and Israel. However, with emerging evidence pointing to a relatively low incidence and transmission rates of COVID-19 among children and the success that many of these countries have had in suppressing the virus, some have started to operate at close to normal capacity with no distancing measures in place, e.g. in France, the Netherlands, Switzerland, New Zealand, and Australia. Denmark and Germany will also be operating at full capacity from August, at the start of their 2020-21 school year. In some countries, schools are also trying to optimise the use of the summer to make up for lost teaching time during the lockdown. In New Zealand and Thailand, the dates of holidays for the remainder of the calendar year have been modified.
In contrast, some countries with some of the highest total number of cases and deaths from COVID-19 are leveraging distanced-learning until they have sufficient time to prepare to operate with full attendance in schools, e.g. Spain and Italy who plan to operate at full capacity from September.
Distancing measures were in place in all countries until very recently. Given the difficulties around maintaining physical distancing, schools have been using innovative strategies to ensure they can keep staff and children well separated (see summary in Table 2, Technical Document 1). These typically involved a minimum distancing length of 1-2m, a maximum number of pupil per classroom, staggered start, finish and break times, one way systems outside of classrooms, assigned desks, and outdoor or off-site learning in places with better ventilation and more space. In Denmark, open spaces, and unused spaces such as a football stadium are being used for teaching purposes. This approach is particularly useful for heavily populated big cities with a large number of children per classroom. It is important to note that these distancing measures are only feasible while most pupils continue to work from home. As countries start to operate schools at full capacity, distancing becomes more difficult and infection rates must be monitored to understand if a setting with no distancing will increase transmissions among children or not.
Multiple other public health measures are being used to suppress the virus. All schools have set-up enhanced facilities for cleaning school property and for regular handwashing, although this no longer being implemented in New Zealand and Australia. In schools that have opened, only Germany, France, Spain and Israel are mandating the use of masks, typically for older age groups or when they are travelling or mixing with others or cannot practice sufficient physical distancing. In Norway, staff members at schools are asked to disinfect classrooms and toys twice a day.
The approach to case management in schools is not entirely clear and, in many countries, appears suboptimal. Evidence to date points to low transmission rates among children, and so most countries are only testing symptomatic children in schools. Symptomatic children are isolated, and, in some cases, authorities are notified, but not always. In contrast, in Israel, a positive case results in the whole school being tested. In Israel and a few other countries, parents have to sign a health form confirming their child and/or family members do not have COVID-19 before being permitted into school. In Beijing, students fill out a survey on an app that calculates their risk of infection. If the risk is too high, they cannot attend school physically. In Shanghai, some schools have designated rooms to isolate students with fever. Other policies are detailed in the tables below and include the use of partitions in classrooms when distancing is not a possibility, e.g. in Spain from September, decluttering classrooms in Australia, not allowing physical contact or toys or lunches to be brought in from home in Israel.
For the schools that have opened at close to full capacity, there is little data on the impact on the transmission of the virus. In all the countries reviewed there have been individual school closures associated with infections in schools, except for in New Zealand. Israel and France have experienced the most serious outbreaks, although the number of new cases (70-300) is relatively low compared to the number of active cases in the UK. In Israel, the clusters have appeared linked to multiple schools across the country resulting in total school closures; some reports suggest that 12% of new cases were detected in a school setting though this does not imply that the school was the source of the infection. A senior source in Israel has suggested that local experts believe that transmission of the virus is typically from adults to children. However, this remains unclear without data stratified by age, and regular monitoring of infections in symptomatic and asymptomatic children.
The partial readmission of children into schools across the globe has mostly coincided with a wider sector reopening e.g. of businesses where employees cannot work from home and increased use of transport. This has made it difficult to monitor the impact of schools opening on infection rates. However, assessing the number of new COVID-19 cases in each country before and after schools opened may give some insight into whether school settings have any impact on the number of COVID-19 cases or not. Although most countries did not experience a significant increase in COVID-19 cases after schools reopened, cases in Israel have more than doubled in the 50-day period since schools opened. The increase in cases has largely been associated with children between the ages of 10-19 years49 (source). Figure 1 below shows the 7-day cumulative number of confirmed COVID-19 cases for 10 different countries50. The x-axis gives the number of days since schools began to open, starting 60-days prior to opening. The overlaid line is a loess smooth of the raw count data. Caution is required in interpreting these plots: most countries implemented incremental openings (for example, in the UK only a small number of year groups started attending on 1 June); other social-distancing measures may have been implemented or relaxed during this time and are not shown; even if within schools transmission is rife, it may take several weeks for an increase in cases to become visible. The plots suggest that school openings have not been followed by a large immediate spike in case numbers, but that the rate of decrease in case numbers may have stalled. Statistically estimating the effect of opening/closing schools on the infection rate has proven difficult, in large part because countries have tended to implement or relax a variety of NPIs simultaneously51.
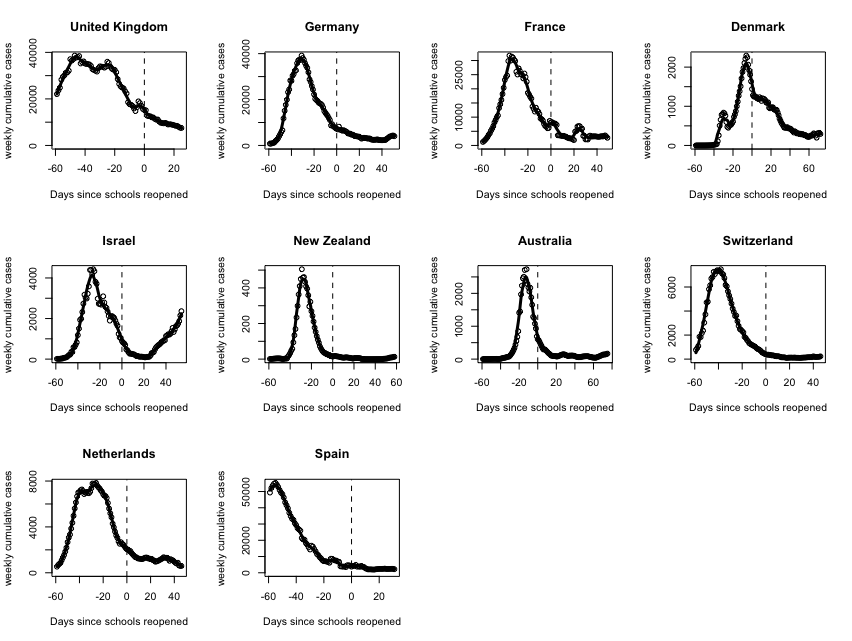
Figure 1. Case numbers following school openings
d. Key Interventions for Schools in the UK
i. Implementing Further School Closures
Although, nationwide school closures were implemented as cases of COVID-19 surged around the world, once pupils were readmitted – typically in phased fashion and with reduced capacity – national closures were not reintroduced. Once the virus has successfully been contained – or better suppressed or eliminated –, then flare-ups are dealt with rapidly on a local scale. For example, in Germany, localised closures are being implemented at varying levels in line with the number of infections. In mid-to-late June all schools and daycare centres in the German district of Gütersloh closed after an outbreak of 400-657 cases at a local meat factory52. In contrast, several schools in Magdeburg, Saxony-Anhalt were closed after an accumulation of approximately 60 new cases in a few days63. In May, a single primary school in Wuppertal, North Rhine-Westphalia was forced to close after new infections were detected53. Finally, in the Bavarian district of Neu-Ulm, 98 children and adults were sent to quarantine after COVID-19 cases were found in three primary school classes and a kindergarten group, but the rest of the school remained open54. Additionally, in Israel, the Education Ministry director-general asked schools to prepare for three scenarios from the start of the school year in September, depending on the number of COVID-19 cases detected55. In the best-case scenario, schools will operate at full capacity. Although, middle schools and high schools will combine in-person and remote learning, while elementary and kindergarten students will continue with the existing framework, with added health regulations. In a second scenario, older students from fifth to twelfth grades will study remotely, while their younger peers in first to fifth grades are divided into smalls groups in schools, allowing distancing to be implemented. Only preschool students will remain in full-size classrooms with enhanced hygiene. Finally, in a worst-case scenario, all children, including pre-schoolers will split into small groups too. Local middle and high schools will be used to accommodate them with additional staffing66.
It is critical that the UK Government provides clear guidance on how schools will manage any future surges in cases and under what circumstances. We have provided an example set of scenarios and actions in the Recommendations section. In some countries reviewed, the criteria for closures and responsibility of decision making is not clear. It is essential that we learn from this and provide clear guidance and determine a coherent chain of command and responsibility to take effective local decisions.
ii. Face coverings in Schools
The use of face coverings or face shields has not been recommended in the Government’s guidance for schools unless children or staff display symptoms of COVID-19 and if “direct personal care” must be administered on school grounds.
Although its use in younger children may not be practical or effective – emerging evidence suggests that there may be less viral transmission from children to adults and that the dominant mechanism in young children may not be from breathing, coughing or sneezing (see section 3b) - its use should be considered for all adults (teachers, non-teaching staff and parents at school) and older children in schools, especially if there is a high rate of viral transmission locally and physical distancing is not possible56. In line with the Government’s guidance, this should include its use if public or school transport is used to travel to school.
The DELVE report on masks published in May recommends the use of face masks or face coverings to reduce onward transmission where physical distancing is not possible, especially in crowded places. This is based on the emerging scientific evidence that shows a decrease in the rate of coronavirus infections where mask-use is compulsory and its usefulness in limiting how far breath can travel24. This advice should not be ruled out for schools.
Although not all countries in our international review appeared to make use of masks or face coverings in their schools, those with a relatively high number of COVID-19 cases recommended its use in areas where distancing is not possible or where mixing outside of class groups occurred, e.g. in some classrooms, hallways and on transport, in for example France, Switzerland and in Israel. More recently, in the US, the American Academy of Pediatrics and the Centers for Disease Control (CDC) have recommended the tailored use of masks and face coverings when schools open at full capacity in Autumn57,58. The CDC has advised schools to teach and reinforce the use of cloth face coverings for staff and children –again, older children in particular – except those under the age of two years, those who are unable to remove the mask without assistance and those with breathing challenges.
There is some concern that the use of masks will impede learning. Research has previously shown that the observation of the face, including the mouth is an important tool for learning and language development59,60. While this is important for young children, the use of face coverings will likely provide greater benefit at less risk to language development for older children in secondary schools.
iii. Winter challenges
The 2020-21 winter ‘flu season will pose challenges for monitoring and responding to possible COVID-19 in schools, and this should be considered in planning for the Autumn and Winter terms of 2020-21.
Firstly, two of the most common symptoms of COVID-19 (namely, a high fever and a new, continuous cough) can also be symptoms of seasonal influenza. Hence, as has been widely recognised61, there is a risk that symptoms of seasonal influenza will be mistaken for symptoms of COVID-19, and vice versa. Other viruses commonly contracted by school-aged children, for example rhinoviruses, can also exhibit symptoms that can be mistaken for COVID-19. This will make monitoring and outbreak response harder in the case of COVID-19, from late Autumn until Spring. For example, a child may contract influenza and develop a high fever or a new cough on the morning of a school day; the child’s parents may then believe (based on the symptoms) that the child is experiencing the onset of COVID-19. If the child’s parents are following NHS guidelines, they will then keep the child at home; they may also telephone the school reporting that the child has COVID-like symptoms. A similar problem could occur if pupils contract influenza and develop symptoms (while at school) which are then mistaken for COVID-19 symptoms, so that they are sent home with suspected COVID-19, whereas in fact they are suffering from influenza. If this happens for several children in the same school, it may be believed (wrongly) that there is a COVID-19 outbreak in the school, possibly precipitating partial or full closure. The problem will exacerbated if there is a delay in such children being NAAT-tested for COVID-19, or if the results of NAAT-testing take longer than 24 hours to be received. On the other hand, there is also a risk that children who contract COVID-19 may be believed (wrongly) to have influenza and not COVID-19, leading to a failure to test them for COVID-19, or a delay in doing so. This could increase the risk of delays in the detection of COVID-19 outbreaks.
To mitigate against these risks, schools and parents and guardians should be provided with adequate and timely NAAT-testing for COVID-19 – to enable prompt testing after a need has been identified, with a rapid turnaround time between testing and getting the results. To do this, the Government will need to ensure that sufficient resourcing – testing kits, labour consumables etc. – is made available in preparation for the winter. There may also be an argument for advising that the result of any NAAT test, when performed for a school-aged child, be reported (along with the school attended by the child) by the testing site (after requesting the parent to provide the name of the school), if at all possible.
Additionally, parents should be encouraged to promptly test children with symptoms and report the results of testing. A COVID-19 winter preparation public information campaign targeting parents and schools should be considered.
Finally, as is argued in the recent report of the Academy of Medical Sciences61, there is also a very strong case for increasing influenza vaccination coverage of primary school children. We further recommend a cost-benefit analysis of widening the eligibility for influenza vaccination to secondary-school children (or certain age-groups thereof).
e. What we need to do
To make decisions about opening and closing schools we need to answer three specific questions:
-
What is the relative prevalence of COVID-19 in children attending and not attending school?
-
What is the effect on the infection rate in children of a policy decision to allow schools to re-open (this will inform future closures and openings)?
-
At what rate does infection spread within schools (both within and between protective bubbles)?
Given that our understanding of the role of children in the transmission of SARS-CoV-2 is still developing, targeted data collection programmes are required if we are to answer these questions. The phased re-opening schools offers an excellent opportunity to address these questions, providing valuable information to inform future decision making. However, low infection rates and other factors make answering these questions challenging from a data perspective. In Techncial Document 2, we discuss what data should be collected, and in particular, how the COVID-19 Surveillance in KIDs (sKID) programme run by PHE could be expanded. We recommend that sKID
-
expands so that as well as testing children attending a school, it also tests children from the same school who are not currently attending (from year groups who are invited to attend, and from year groups who are not)
-
tests at least 13,000 children attending school, and 13,000 children not attending for four consecutive weeks, in order to have sufficient statistical power to detect an increased prevalence within schools
-
include an element of responsive testing: positive diagnosis of school children should be followed by tests of other children/staff from within the same school in order to understand disease transmission within schools, and possibly from others living with these children in order to better understand the risks to cohabitors of living with infected children
-
continues to test children isolated from school after a positive test within their bubble.
Our analysis suggests that the current design of sKIDs means that the programme is unlikely to answer crucial policy-relevant questions. We also note that surveillance studies such as sKID require huge sample sizes to be effective when infection rates are low, and so responsive testing and detailed case study analysis of test results (including of phylogenetic data) from schools which have experienced an infection, may be a more feasible approach to understanding transmission in schools.
The statistical design needed to understand the dynamics of COVID-19 transmission in schools is explored in further detail in Technical Document 2.
3. Learning loss from school closures
There are two stages to this: first, estimating the learning loss, and second, estimating the implications of that for outcomes of interest such as life chances, earnings, health and mortality.
a. What we know
i. Estimates of expected learning loss
Even a relatively short time in school increases a child’s cognitive ability; even a relatively short period of missed school will therefore have consequences for skill growth. Missing twelve weeks of school is likely to have a very significant impact. The impact is likely to be greater for younger children, given evidence that investments in children’s learning tend to be complementary over time – having higher levels of skill in the first period makes it easier to learn more in the second period for a given level of investment (e.g. teaching time)62. This implies that time out of school is likely to have a bigger impact on younger children’s cognitive skills.
There is an existing literature on the impact on learning of school closures. It is important to note however, that the current lockdown situation is unprecedented and therefore existing evidence can only be taken as a guide to study the magnitude of the impact on attainment loss and gap.
The key methodological challenge is that estimating a causal impact of school time on skills requires a setting with exogenous variation in the former. Consequently, the most robust evidence covers the effects of school closures because of teacher strikes, weather extremes, and other quasi-random settings. For example, Carlsson et al (2015)63 use conditionally random variation in school time to prepare for a test in Sweden, and show that 10 days of additional learning time increases test score measures (of knowledge/crystalised intelligence) by 1% of a standard deviation. Lavy (2015)64 explores the impact of cross-national variation in hours of instruction and found an additional hour of instructional time in a subject per week over the school year was associated with a gain in test scores of 6% of a standard deviation. Burgess and Sievertsen 202065, drawing on the above literature, estimate that both of these papers imply that the loss of 12 weeks of schooling suggests a loss of 6% of a standard deviation in test scores. Goodman (2014)66 show that for every 10 days of absence due to extreme weather (here, snowfall) in the US (Massachusetts), mathematics scores reduced by 5% of a standard deviation. Aucejo and Romano (2016)67 find a decline between 5% to 10% of a standard deviation in mathematics score for students in the US (North Carolina) in the case of absence due to flu. Cattan et al. (2017)68 use sibling differences in data from Sweden to try and isolate the effect of school absence. They find a moderate adverse effect of absence, which fades out by mid-adulthood.
There are catastrophes that have generated useful data and insights to guide us. For example, the educational impact of Hurricane Katrina in New Orleans in 2005 has also been studied. The immediate damage was catastrophic; in addition to around 1900 lost lives, 110 out of 126 public schools were completely destroyed, and the children who survived the storm displaced to other states for the rest of the school year. The immediate negative effect on test scores was substantial. Sacerdote (2012)69 finds “reasonably large (7%SD to 20%SD) declines in test scores for all students who are displaced by the hurricanes”. Interestingly, test scores of these students subsequently recovered partly because students were relocated to much better schools (necessarily so, because it was the poorest schools which were worst hit by the hurricane) and partly because of wholesale reform of the New Orleans public school system. Whilst this might give us hope that remedial action is possible, minimising the loss in the first place is obviously a priority.
Others are more sanguine about the impact of the loss of twelve weeks of schooling on educational outcomes. Hattie (2020)70 suggests “Do not panic if our kids miss 10 or so weeks [of school]” (p. 1), though he also states that the “most likely implication of school closures relates to equity”. He cites as support that the pupils affected by the earthquake in Christchurch New Zealand did not suffer much reduction to their end-of-year test scores; this is documented in Beaglehole et al (2017)71, though they also note that education was disrupted rather than closed completely.
Finally, a different literature has documented the phenomenon of “summer learning loss”: the view that students fall back in their learning over the long summer break in the US. The most comprehensive systematic review of estimates of summer learning loss is Cooper et al. 199672 who draw on evidence from 39 (largely US) studies and undertake a meta-analysis of the results from 13 of them which meet minimum criteria. Aspects of the methodological rigor of the evidence on summer learning loss have been called into question by the issues raised in von Hipple and Hamrock (2019)73. This scepticism74 about the classic findings of summer learning loss, with inconsistencies in estimates from different studies, partly related to faulty research design, means that that evidence is now seen as questionable. More recently, Atteberry and McEachin (2019) 75 document the huge diversity in learning loss, taking account of the measurement issues, with a relatively small group of students accounting for a lot of the “loss”.
The second part of the story is to estimate the later impacts of the lost skills if they are not remediated: lower skills have implications for individual lives and for the economy as a whole. First, a huge base of evidence shows that earnings depend on skills, and lower skills means lower earnings. Second, those lower earnings are reflected at a national level in lower growth. Third, there is a link to health and to mortality, so that in a general sense the risk of death from infection can be compared to the risk of death from poverty.
The most important implication for an individual is lower earning potential. Higher skills command higher earnings. As Portes (2020)76 succinctly puts it, if a student misses a quarter of a school year, and each school year brings roughly a 10% return, earnings potential is likely to be permanently lower by around 2-2.5%. That loss is likely to be higher if the disruption happens early in an educational career. Of course, education matters causally for other outcomes in adulthood too, and these are likely to be compromised by the lost skills: health and longevity, unemployment, and wellbeing among many. Jaume and Willén (2019)77 exploit cross-cohort variation in the prevalence of teacher strikes in Argentina and show that exposure to average strike incidence in primary school reduces earnings in mid-life for women by 1.9% and for men by 3.2%, as well as raising unemployment.
At the national level, lower aggregate skills will reduce the growth rate. The magnitudes are not trivial: 13 cohorts of students have been affected by the lockdown, so from the mid-2030s, all workers in their 20s will potentially have lower skills than they would otherwise have. And for the 50 years following that, around a quarter of the entire workforce will have lower skills, with a consequently lower growth rate. The present value of such a fall in the growth rate is measured in billions not millions. Turning again to Jaume and Willén (2019)77, they estimate the aggregate earnings loss in Argentina from lower skills if $2.34 billion per year.
As well as a fall in income, all the evidence to date points to a widening of inequality. This issue is discussed in detail below and clearly will have further stark consequences for individual livelihoods and for social cohesion.
One of those consequences is the impact on health and life expectancy. Low earnings from skill loss can be expressed differently as a much greater risk of poverty. For example, the ONS states that “In the UK, those with a low level of educational attainment are almost five times as likely to be in poverty now as those with a high level of education”, and “Holding all else equal, in the UK, those with low attainment are 11 times as likely to be severely deprived as those with a high level of education”78. There is a huge literature linking poverty to ill health and early death, though isolating a causal relationship is always tricky. For example, Bennett et al (2018)79 report a 7.9 year gap in life expectancy for women and a 9.7 year gap for men between the most and least deprived deciles of areas poverty in 2016. Linking more directly to outcomes for children, and again representative of a large literature, Cattan et al (2019)80 show in a plausibly causal approach that access to Sure Start Sure Start reduced the risk of hospitalisation among primary school children, and that the health benefits grew bigger as the children got older.
In summary, the skills loss from missing school is not trivial, and is likely to lead to lower earnings, higher risk of poverty and unemployment with impacts on health and life expectancy.
ii. Variation in learning loss
The actual loss of learning in the current pandemic will vary by context, depending on what schools and families have been able to provide in the way of remote schooling. It is also important to note that attainment gaps prior between different groups of students were a major issue prior to COVID-19 and specifically the gap between students from low and high socio-economic status families. A priority is therefore to provide evidence on the extent to which learning loss might be worse for some groups, particularly socio-economically disadvantaged students (see also Sims 2020, Montacute 202081; Burgess and Vignoles, 202082).
The Education Endowment Foundation (EEF) 202083 report presents a meta-analysis of the existing literature, focusing particularly on studies that provide estimates of changes in attainment gaps between low and high SES students during the school year and over the summer. This evidence therefore provides useful quantitative data on the likely impact of school closures on the attainment gap between disadvantaged pupils and others. The EEF meta-analysis also includes a detailed critique of the methodological problems with some of the summer learning loss literature (see also von Hippel and Hamrock, 201984).
A table from the EEF report mentioned above, reproduced with their kind permission, provides 15 key estimates of the impact of school closures on attainment gaps from 9 studies (see Appendix).
For most studies, school closures of various descriptions worsened the rate of change in the attainment gap, ranging from increasing it by 0.113 standard deviations per month in reading scores evidenced from a study in Germany (Meyer et. al, 201785), to 0.009 standard deviations per month in mathematics scores evidenced from a study in Sweden (Lindahl, 200186). Two similar US studies (Dumont 202087 and Quinn et al. 201688) actually showed a decline (albeit very small) in the attainment gap between the rich and poor due to school closures, for both reading and mathematics, by 0.021 and 0.001 respectively. The EEF study calculated the average rate of change in attainment gap to be 0.022 or 2.2% of a standard deviation per month (EEF 2020). By their calculations, school closures will widen the attainment gap by between 11% and 75% by September 2020, with a median projection of 36%. The study also caveats that the projections might be an overestimate for those students who have returned to school or who will be returning to schools earlier than September, and for those students in schools where remote schooling has worked well.
Another group potentially at greater risk from school closures is students from BAME backgrounds. In terms of academic achievement measured by GCSE scores, the latest Department for Education figures from 201889 show that Chinese, mixed and Asian groups of students continue to perform above the national average, whilst White and Black groups remain below. These broad groupings hide variation and some groups, such as Gypsy/Roma and traveller of Irish heritage students, have much lower achievement than others. Further, ethnicity intersects with low income, particularly for BAME groups. Among low income students, many minority ethnic groups have higher levels of academic achievement (as measured by GCSE scores) and make more academic progress during secondary school than White British students. However, Black Caribbean boys perform at a similar level to White British students90. Among high income students by contrast, White British students outperform all minority ethnic groups bar Indian students. In terms of academic achievement therefore, it is not the case that all BAME groups are at risk of low achievement pre COVID-19. Whether this continues during the pandemic depends on the quality of remote schooling and support from parents, and whether that varies across ethnic groups.
Of particular cause for concern is the fact that while students from BAME backgrounds make up twenty-nine percent of the students in England and Wales, they account for a disproportionate amount of the school exclusions. Mixed White and Black Caribbean pupils had particularly high exclusion rates and were both nearly three times as likely to be permanently excluded as White British pupils91. Out of all ethnic groups, pupils from Black and Mixed backgrounds had the highest rate of temporary exclusions. In 2014/2015, 250 Black Caribbean pupils out of 5,770 pupils were permanently excluded from school92. There is also a large literature on the racism experienced by Black Caribbean students in particular, putting them at risk of exclusion and disengagement93. Reports of punishments being related to race are widespread. The Independent recently reported, “schools are unfairly punishing Black students for their hairstyles, wearing bandanas and kissing teeth” due to racial bias and general lack of understanding94. Previous studies have also shown that school absences and suspensions have been linked to lower test scores and lower school performance. If school closures lead to some students who are already at risk of exclusion and/or high absence rates falling still further behind, they may become even less engaged on their return to face to face schooling. We might then expect an exacerbation of these issues in academic year 2020/21.
Some BAME groups are also at much greater risk of having low income which will impact on families’ ability to support children during the pandemic. Even amongst highly educated individuals there are significant differences in earnings by ethnicity. Among graduates for example, while Indian and Other Asian ethnic groups had the highest average (£28,500) earnings five years after graduating, Black and Pakistani ethnic groups had the lowest average earnings five years after graduating (£22,400)95. At the other extreme, according to the Office of National Statistics, children in Bangladeshi and Pakistani households were most likely to live in low income and materially deprived areas out of all ethnic groups96. Children living in poverty are more likely to have lower levels of educational outcomes and, as discussed in the next section, more likely to experience learning loss during the pandemic.
iii. Variation in schooling and home support during the pandemic
It is important to understand why school closures are likely to have impacted on children’s learning and specifically why they might have widened the socio-economic gap in achievement. There are two main mechanisms. First, household income and family environment are major determinants of children’s academic achievement in normal circumstances. The pandemic is likely to have exacerbated the effects of these determinants of learning, not least because there is some evidence that socio-economically advantaged parents tend to compensate for any deterioration in schooling to a greater extent. Second, remote schooling might be less effective than face to face schooling, particularly given that schools had to switch to remote schooling very rapidly in March without any preparation.
We do have some current data from the UK to illuminate us on the first issue. A recent brief from The Sutton Trust97 reports findings from a Public First survey conducted between 1-3 April 2020, on a sample of 1508 parents with children aged 2 to 18, weighted on the basis of gender, SES and region to represent the entire population. The report suggests that during this crisis 44% of middle class parents are spending more than 4 hours a day on home schooling. One third of working class parents are doing so. Note also that this survey was conducted early on in lockdown and we might expect that many parents will have been able to spend less time supporting their children as lockdown persisted and expectations from employers increased. Moreover, middle and higher income households are, unsurprisingly, more likely to spend money (>£100) on their child’s learning during the lockdown (19%) compared to working class households (8%). Data from this Sutton Trust survey also suggested that pupils in independent schools were more than twice as likely to be experiencing online teaching during lockdown. For example, only about one in five children in state schools were taking part in live and recorded lessons on a daily basis. In independent schools, just over half of students were accessing online lessons daily. This is perhaps partly attributable to the fact that whilst 60% of state schools already had an online platform of some description prior to lockdown whereas only 37% of state schools had one.
Andrew et al 202098 report similar findings from an online survey of 4000 parents with children aged 4 to 15, conducted by Institute for Fiscal Studies and Institute of Education between 29 April-12 May 2020. The sample is weighted to provide an England wide picture. Children in the richest quintile of families spend over 75 minutes per day more on school work than children in the poorest quintile of households. This quickly accumulates: over the (at least) 34 days that schools will be closed, this difference adds up to more than seven full school days. For some year groups, particularly those nearing the end of schooling, this might have a major impact on their attainment. The report also finds that students from more affluent families are more likely to have access to private tutoring, individual discussions with teachers, access to technology and online resources. All three of these resources are likely to ensure that high SES students are better able to gain from remote learning.
The evidence on the impact of remote learning techniques as a substitute for face to face teaching is rather limited, particularly in the context of primary and secondary school pupils. Prior to the pandemic, online learning was only prevalent in higher education and has been characterised by high levels of drop out from courses. Moreover, during the pandemic, the provision of remote teaching has been highly varied across schools, both in terms of quantity and quality.
The most comprehensive data on what schools are currently offering to support remote learning comes from a recent National Foundation for Educational Research (NFER) report99, which presents headline findings from an England wide survey of 1,233 senior leaders and 1,821 teachers from primary and secondary schools (weighted to represent the population). The survey focuses on school provision, pupil engagement in remote learning and the factors that affect it. This survey represents nine per cent of primary schools and 20 percent of secondary schools in England and further longitudinal follow ups are planned100.
NFER have kindly shared early findings with us and full details can be found in Julius and Sims (2020), Lucas et al. 2020 and Sharp et al. 2020101,102. Findings include:
-
In May 2020, teachers reported being in regular contact with, on average, 60 percent of their pupils. However, less than half of pupils (42 per cent) returned their last piece of set work.
-
Most teachers (80 per cent) reported that they were covering less of the curriculum with their classes than usual.
-
Most teachers (90 per cent) believed that their pupils were doing less or much less work than they would usually expect at this time of year.
-
Teachers reported that the following proportions of pupils are less engaged than their classmates: pupils with limited access to IT and/or study space (81 per cent); vulnerable pupils (62 per cent); pupils with special educational needs and disabilities (SEND) (58 per cent); pupils eligible for Pupil Premium funding (52 per cent); and young carers (48 per cent).
-
Pupil engagement and disadvantaged pupil engagement were both lower in the most deprived schools. Teachers in the most deprived schools were in contact with fewer pupils.
-
Teachers reported that, on average, just over half (55 per cent) of their pupils’ parents were engaged with their children’s home learning. Parental engagement was significantly lower in the most deprived schools (41 per cent) compared to the least deprived schools (62 per cent).
-
The proportion of pupils with little to no IT access in the most deprived schools (39 per cent) was double that of the least deprived schools (19 per cent). Teachers in the most deprived schools were also more likely than those in the least deprived schools to say that all areas of the curriculum are currently getting less attention than usual.
-
Schools using a virtual learning environment (VLE) to inform pupils about learning activities – rather than the school website, and those delivering learning content to pupils through online conversations or activities that involve consolidating previous learning or revising, had higher pupil engagement levels and an increased probability of having highly engaged disadvantaged pupils.
-
Three-quarters of senior leaders reported that their schools were offering ‘social or welfare’ support to vulnerable pupils, often by working with other agencies. For example, many schools were supporting their pupils by providing food vouchers and parcels (95 per cent) and providing non-education related information (83 per cent) to assist families.
-
There were greater concerns about the welfare of vulnerable pupils in the most deprived schools: 54 per cent of senior leaders in these schools reported significant concerns for the safety and wellbeing of vulnerable pupils, relative to 35 per cent of senior leaders in the least deprived schools.
-
Leaders from schools with the highest proportion of FSM pupils were more likely to report that they had experienced a significant drop in numbers of pupils attending school before 20 March (73 per cent) than those with the lowest proportion of FSM pupils (56 per cent). This suggests that disadvantaged pupils may have been missing school before the lockdown.
-
In May, senior leaders reported that they had only 75 per cent of their normal FTE teaching capacity available: 53 per cent to work in schools and 22 per cent to work at home only.
Overall, this research suggests that students from the most deprived schools are less likely to be engaged in remote learning compared to those from more affluent schools, that teachers are very concerned about lack of engagement in remote learning for about a quarter of their students and that little or no access to IT is an issue.
The EEF have also published a rapid evidence review of 60 review studies to investigate the effectiveness of various remote learning methods including distance learning, blended learning, computer assisted learning and educational games. Their review covers all age groups of students103. The report summarises key findings and also appraises the methodological rigour of the evidence base. While acknowledging the limited number of studies which are directly applicable to school age pupils, the results suggest nil or only limited impact on outcomes from remote teaching compared to traditional teaching. For example, Means et. al, 2013104 found no significant difference in student outcomes when comparing purely online vs traditional face to face teaching. However, studies that compared blended teaching (online combined with face to face) with just face to face teaching, on average found a positive impact on learning outcomes from the former.
One of the most common forms of learning during the current pandemic has been the use of “apps” - mobile based applications which also give adaptive feedback to students. The EEF review of 29 studies focusing on the effectiveness of computer assisted learning found that most of the review studies showed an overall positive impact from this technology, ranging from a 75% improvement in vocabulary test scores, evidenced by Chiu 2013, to a 9% improvement in mathematics learning outcomes, evidenced by Steenbergen-Hu and Cooper 2013. Only one study showed a negative impact, specifically a 26% reduction in reading scores as evidenced by Strong et al., 2011.
Overall there is insufficient evidence to date to guide us on the expected impact of remote schooling on learning. However, most studies do not suggest that online teaching is, in and of itself, likely to have a major negative impact on learning. However, this finding may not hold if the online teaching is of poor quality, which may be the case given the speed at which schools were expected to adapt to it. Nor will it hold if students are unable or unwilling to actively engage with it, as seems to be the case for many. Further, the EEF review did not uncover any studies that measured the effectiveness of computer assisted/online learning on disadvantaged students’ learning in particular. Since access to technology is a major challenge for such students, we need more evidence on this issue.
Certainly at a practical level, there have been growing concerns about uneven access and availability of inputs into education (for example, computers, laptops, online resources, private tutoring) and its impact on learning outcomes. Access and provision to these vital resources varies across socio-economic groups and across schools. Andrew et al, 2020105 find rich parents were 15% more likely to report that their child’s school offers real time online classes than their poorer counterparts. They also find children from poor families were only half as likely to have access to private tutoring compared to their richer peers.
It is also worth noting that even when schools open, there may be ongoing issues regarding differences in schooling experienced by children from different socio-economic backgrounds. In the period leading up to lockdown, schools reported that not all their students were attending. Further, it appears that students from more socio-economically disadvantaged backgrounds were less likely to attend school in the period just before lockdown. For example, the National Foundation for Education Research survey106 reported that 61% of school leaders reported a significant fall in the number of pupils attending school prior to 20th March (the date schools closed). School leaders in schools with the highest proportion of Free School Meal pupils reported a far larger fall in the numbers of pupils attending school (73% decline) compared to those in schools with the lowest proportion of FSM pupils (57% decline). The Institute for Fiscal Studies survey of parents in May 2020107 found that only 39% of primary school parents and 45% of secondary school parents were planning to send their children to school when they reopened. Further, higher income parents were more likely to say that they would send their children to school than lower income parents. As of week commencing 11th June 2020 in schools that were open, only 32% of reception children were actually attending, 29% of year 1 students were attending and 39% of year 6 students were attending108. Persuading parents to send their children to school, particularly those from low socio-economic status backgrounds, may be a challenge though the Government has announced that in September usual sanctions can be applied to parents who do not send their children to school.
b. What we need to do
We do not currently have direct measures of children’s learning loss as a result of the school closures. This is clearly a major data gap. The first step is therefore to collect the necessary test score information needed to estimate the scale of the learning loss from school lockdown. While we have good data current on “inputs”109 into home learning (for example, parental time and ability, school provision, and availability of IT kit), there is currently nothing available on “outputs”.
Outputs of the skills formation process are typically measured by achievement tests. These might be one-off high-stakes tests such as GCSEs, non-qualification but internally-important school tests, or recurring low-stakes tests on online learning platforms. In the present pandemic context, such measures are rare: all qualification tests have been cancelled, and most schools understandably appear to have cancelled internal tests. And yet, such data are key to quantifying the risk from keeping schools closed.
An ideal design to properly gauge the learning loss from lockdown would take a difference-in-difference design: use a robust measure of pupil achievement both pre- and post-lockdown, and for pupils who were and others who were not kept out of school. However, since all schools closed110, this approach is simply not possible. Second best would be to look just at the longitudinal aspect and compare the distribution of equivalent test scores before and after school lockdown. Understandably, it appears that very few schools are testing pupils as this report is written (late June 2020), so the first date of general testing will be the general return to school in September. Because there is no national, officially-sanctioned test for all age groups111 at that date in the UK, we recommend an additional test at the beginning of the school year, and then again at the end of the school year to measure any catch-up during the year. The burden on schools now and more so in September will be large, so we also recommend that these tests be carried out on a sample of schools rather than be universal.
The second problem we face is that while the exercise could be carried out using bespoke tests, for many schools there would be no comparator for the previous cohort, the “before” benchmark. In this case, we recommend using tests that have a ‘synthetic’ before score – that is, normed tests that have a known and validated typical score in normal times112. These norms can act as baseline, ideally differentiated by some basic demographic controls. The limitation of this approach is that these age-normed tests are not closely aligned with the curriculum and may instead tend to measure students’ general ability and hence understate the extent of specific learning loss related to the curriculum. The age-appropriate tests would be taken by pupils of all age groups in school in September 2020 in samples of schools; ideally, we would pick different schools per age group to sample a wider range of school effects. Prior to detailed power calculations, a rough order of magnitude based on typical ICC estimates would be around 150 secondary schools per age group, and perhaps 600 primary schools per age group. It may well be that the UK Department for Education will want to carry out such tests to gauge the depth of learning loss, and it would obviously be productive to confer.
Another, more informal and ad hoc approach, is to collect data from schools that are using their own internal tests to assess the progress of their students, for example using online learning platforms. One powerful example of this is Goldstein113 reporting work carried out by Chetty and team at Track the Recovery114.
We have been able to access some similar data for the UK; as far as we know, this is the first time that outcome data for the period of the Covid-19 closure has been analysed to show the impact of the lockdown in the UK. This data is from an online learning platform, where young people between the ages of 5 and 16 from subscribing schools can take Star tests on reading and understanding. We are grateful to Renaissance Learning for providing anonymised pupil and school test data for this report, including a pupil ID reference that is used for internal Renaissance purposes only, a date of test, minutes spent per test, and the test scores. In all, around 160,000 data points were provided for the period September 2019 through mid-June 2020. There is no generally set time frame for taking the tests so a week-by-week or month-by-month analysis might be misleading: for example, it might be that the more able students tend to take tests later in the year. But clearly, one very salient factor for test taking will be the school lockdown and the strong encouragement from schools to use online resources. So, we simply look at the distribution of test scores before and after the lockdown, for a fixed set of pupils who take tests 1 or 2 times pre lockdown, and also take tests 1 or 2 times post lockdown. This is designed to reduce the scope for selection issues to drive the results. Figure 2 plots the interquartile range for this group shows that the difference between the scores of high-performers and low-performers increases markedly after the schools lockdown. This is particularly clear for primary school children, less so for secondary school children. To scale the IQR, the pre-lockdown average scores were respectively 378 (for year 3), 541 (year 5), 734 (year 7) and 870 (year 9). Figure 3 provides more detail in the form of a QQ plot.

Figure 2
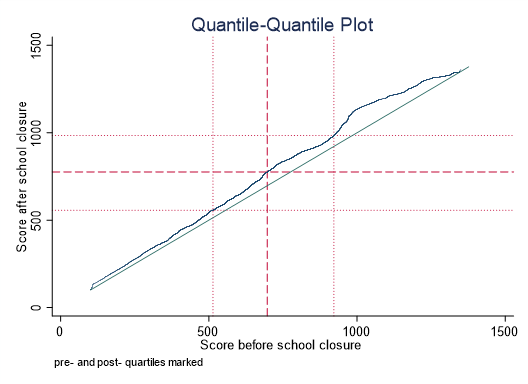
Figure 3: QQ Plot
This picture fits well with the increased inequality seen in learning inputs over the lockdown period, and is concerning for the future learning outcomes for these cohorts and their life chances beyond education.
4. Measures of other losses
In this section we consider some of the other impacts from school closures, beyond infection and learning.
Our response to COVID-19 has had an acute economic and social impact. For example, the impact on unemployment and household income has been immediate115, though clearly muted due to the furlough scheme in the UK. To give some sense of scale, data from the Office for National Statistics suggests a 69% increase in the numbers claiming unemployment benefit between mid-March and mid-May116. In the medium term we are anticipating further significant loss of economic activity and accompanying job losses. These worsening economic conditions will have major impacts on households and hence on children and young people, not least by increasing poverty rates.
The long run relationship between poverty in childhood and adult physical and mental health is well documented. Indeed, the UK had already seen an increase in health and mortality inequalities prior to COVID-19 following the 2008 Great Recession117,118. COVID-19 is likely to exacerbate such inequalities. Any further reductions in household income will also tend to have a causal negative impact on children’s achievement and wellbeing. As an illustration, a recent estimate suggests that an £860 increase in household income results in gains in cognitive test scores of around 5-27% of a standard deviation119. Further, unemployment and reductions in household income are highly stressful for parents (e.g. recessions are linked to increases in suicide rates120,121). Parental stress also impacts directly on child wellbeing. For example, the 2008 Great Recession, and the economic uncertainty it caused, was associated with an increased risk of child abuse and harsher parenting by mothers122. For those families experiencing economic hardship themselves due to job losses etc., there was also an increase in child neglect. Of course, the impact of the current economic conditions will also depend on the Government’s policy response to it. Any reductions in the level of public services available as a result of the more difficult macroeconomic situation will impact further on children and young people, not least via reductions in the quality of health and education provision.
However, these general effects from COVID-19, whilst very relevant to children, are not necessarily directly related to school closures. In this section we review evidence that might inform our understanding of any direct impacts from not having face to face schooling.
a. What we know
Remote schooling is likely to impact children and young people differently, depending on their age and stage of development. Early in the outbreak, psychologists and medical practitioners recognised the substantial risks from school closures and social isolation in terms of their potential negative impact on children’s physical and mental health123,124,125,126,127,128.
In terms of physical health, levels of physical activity are likely to be lower as a result of remote schooling even without additional physical distancing rules, since children tend to be less active out of term time. Sleep patterns and diets have also found to be worse when children are out of school. Growing levels of obesity among children are a risk, since children tend to gain weight when out of school129,130.
Previous health crises have also suggested that procedures such as quarantines have a negative impact on children’s psychological health and risk of post-traumatic stress disorder131. A systematic review by Loades et al. is also relevant to this issue. It reviewed 63 studies that reported on the impact of social isolation and loneliness on children and young people’s mental health. Most studies were observational and there was risk of bias132. However, the conclusion was that social isolation increased the risk of both depression and anxiety both during and after the period of isolation.
In normal times, children benefit from strong attachments to other adults, often teachers, from feeling that they belong at school, and from their relationships with peers133,134. Social competence, autonomy and relatedness are all important to children’s wellbeing and schools play a key role in fostering these135. By implication, this suggests that not being in school will reduce wellbeing for many children.
Social interactions and relationships are particularly important for adolescents. Adolescents who feel lonely and less connected to other people have poorer physical and mental health136. For example, socially isolated teens were found to have poorer cardiovascular health in young adulthood137. Orben, Tamova and Blakemore have argued in The Lancet that social distancing and being socially isolated as a result of undertaking remote schooling, is a particular risk for adolescents138. Specifically, it is a period during which young people have a greater sensitivity to, and need for, social connection and interactions with peers139. The school environment is obviously vital in providing this. Adolescence is also a period of onset for many mental health conditions. Combining unprecedented social isolation with a critically important development period puts these young people at increased risk of mental health problems.
There have also been reports in the media regarding an increase in suicide rates among children and young people. Suicide and self-harm among children and young people has increased since 2010140141 and social isolation has been identified as a potential risk142. However, official statistics on suicide lag and cannot yet be used to determine whether or not there has been an increase in child and young people suicides during the pandemic. Real-time surveillance of child suicide is one way of tracking the problem but obviously comes with caveats as it is not based on official statistics. The National Child Mortality Database has constructed a real time measure of likely suicides in children and young people under the age of 18 over the period January to May 2020143. This covers the first 8 weeks of lockdown from 23rd March to 17th May. They could not find any statistically significant trend given the small numbers involved, though they noted that the number of cases had increased on the previous year.
It is important to also note the risk that on re-opening, schools and education policy might overly focus on the learning loss from school closures at the expense of considering psychological impacts. Since mental health and academic achievement are also closely related, one needs to consider and address both these issues simultaneously144,145. Even before COVID-19, the UK had a growing problem with mental health among children and young people. Around 1 in 8 school-age children had clinically impairing mental health conditions and up to a quarter of older teen girls (16-19 year olds) reported such conditions146. There is also agreement that children or young people with pre-existing mental health problems are going to be, on average, at higher risk during the pandemic. Hence a holistic view of the potential costs of remote schooling is important. Overall, the combination of social distancing, physical restrictions on movement, and school closures leading to a lack of routine and limited contact with other adults and peers, are all likely to negatively impact on children and teens.
Evidence on the prevalence of these problems during the pandemic is still limited but there is some useful data on child and youth mental health and on the impact of lockdown and school closures on parents’ time use and their paid work, which we review below.
i. Impact on child health
Early evidence from during the pandemic suggests that children do report that they miss being in school. It is young people (adolescents) who are least keen on remote schooling, with some signs that younger children also enjoy being in their home environment147. More generally, there is a growing body of evidence suggesting that children and young people have suffered worsening mental health during the pandemic148,149,150,151,152. The Children’s Commissioner instigated a survey of children and youth in March 2020 (n=2000) and also found a decline in young people’s reported life satisfaction and wellbeing, with both children and young people reporting negative impacts from social isolation153. Emerging Minds surveyed parents, carers and adolescents about their mental health and behaviours154. The sample is a convenience one and is not nationally representative. The evidence emerging from this survey is mixed. Parents reported an increase in behaviour and attention problems among primary school age children, and an increase in attention problems among secondary school children. Yet parents also reported a reduction in their children’s emotional problems. Adolescents did not report significant changes in their behaviour or emotions. Such data are potentially problematic to interpret however, not least because they are not nationally representative. Further, it is difficult to identify the impact of school closures specifically, since it is impossible to separate out the impact of remote learning on children and young people from the impact of the greater levels of social distancing required more generally (though they are clearly related).
It is also obviously the case that some children are more vulnerable and at risk of both mental health problems and physical abuse than others, for example children in care155. There has been a documented rise in domestic accidents among children and concerns that child protection procedures are not working as effectively, with children not being properly assessed in terms of their risk156,157. A recent survey of vulnerable young people themselves158 indicates that these young people who were already at risk think that their mental health has deteriorated. They have growing fears and concerns about a range of issues, including health, the impact of school and university closures, lack of social contact and in general the loss of routine. Among those with greater vulnerabilities, a NSPCC survey159 of those in counselling suggests that poor relationships are a major issue for some young people, as well as very difficult family circumstances, potential abuse and difficulties engaging with school work. Further, children with specific conditions, such as neurodevelopmental difficulties like Autism, are also reporting greater levels of anxiety160,161.
Given the additional risks arising from our response to COVID-19, lack of access to public services, particularly in the area of mental health, is a major concern162. The Coronavirus Bill reduced the statutory requirement for some services163 and many services have also moved online, which is unlikely to be optimal. Evidence on the scale and impact of reductions in services is limited however. The YoungMinds survey mentioned above found that around one quarter of young people with a pre-existing condition reported that they were unable to access mental health services, though the survey is not nationally representative164.
Another issue affecting children’s health that has arisen during the pandemic is food insecurity165, which is a problem that predates COVID-19. For low income families experiencing food insecurity, schools provide a vital component of their children’s daily food via Free School Meals. Although Free School Meals are now being provided to children remotely, there was a period early in lockdown when they were not. Children potentially experienced food scarcity during this period. Robust medical data on malnutrition experienced by children during the pandemic is lacking. However, The Food Foundation undertook a survey early in the lockdown. This was the period during which Free School Meals were unavailable and there were significant shortages of some food in shops166. They estimated that the proportion of families with children experiencing food insecurity during the lockdown increased from 5.7% to 11.0%. Further, just under a third of adults with children eligible for Free School Meals reported food insecurity over the period, compared to just one in ten adults with children who are not eligible for FSM.
ii. Ability of parents to return to work
Schools being closed has also had implications for parents167. Although the primary purpose of school is not to provide childcare, it has become apparent during the pandemic that parents do rely on schools for this purpose. If most children are not in school, their parents must undertake childcare and ideally support their home schooling. This is only feasible for those who work at home. For other parents, school closures will significantly impact on their ability to undertake paid work.
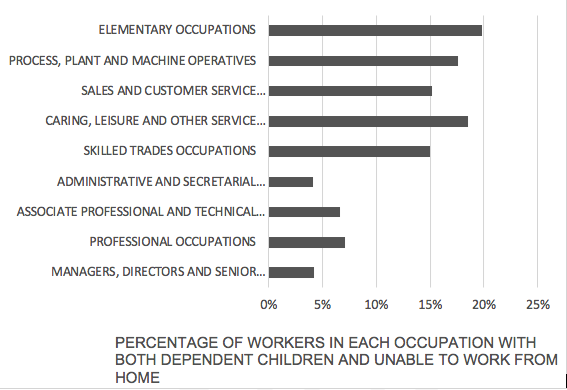
Figure 4
Source: This chart is derived from data kindly provided by Monica Costas Dias using Labour Force Survey 2019. A full discussion of the constraints regarding working from home is further discussed by the IFS168.
Figure 4 shows the proportions of people in different professions who are “constrained” in terms of being able to do their jobs, which is defined as having dependent children and not being able to work from home. Hence one in five of all workers in elementary occupations have dependent children and are unable to do their job from home. This constraint implies they may not be able to go back to work if schools (or some form of childcare) do not open or if there are repeated closures. As can be seen, there is a clear divide between more high-skilled, well paid professions, where a far lower proportion is constrained due to being better able to work at home.
We can therefore infer that the low-skilled will be most constrained if schools fail to open or are subsequently closed. Without government intervention, this group will suffer disproportionate income losses as a result of closures. Further, those with higher salaries may be better able to fund alternative childcare, exacerbating this difference.
The twin effects of the pandemic on work and schooling have also affected women particularly badly, and potentially reversed progress towards greater gender equality169,170. Women are much more likely to work in the service sector which has been largely shut down (Figure 5), reducing their employment and earnings. Since work experience is very valuable in the labour market, an extended period of time with no work may damage their future job and earnings prospects171172. Women are also less likely to have jobs that can be done at home and this means that they are less likely to be able to continue to work during lockdown. The evidence is also clear that the closure of schools and nurseries has meant far greater caring burdens at home. Historically such caring responsibilities have tended to fall disproportionately on women, with implications for the disruption to their paid work173. Evidence from data collected during the pandemic confirms that women have been doing a disproportionate amount of the child care. Among couples where both parents are working, half of the hours that mothers work at home are combined with childcare, compared with just 30% of fathers’ hours174. Single mothers have felt these pressures even more strongly, unable to share childcare and home schooling, and typically being in lower paid jobs to start with. It is perhaps noteworthy that Understanding Society data also suggests women have been experiencing higher levels of psychological distress, which appears to be attributable to additional hours of childcare and home schooling175.
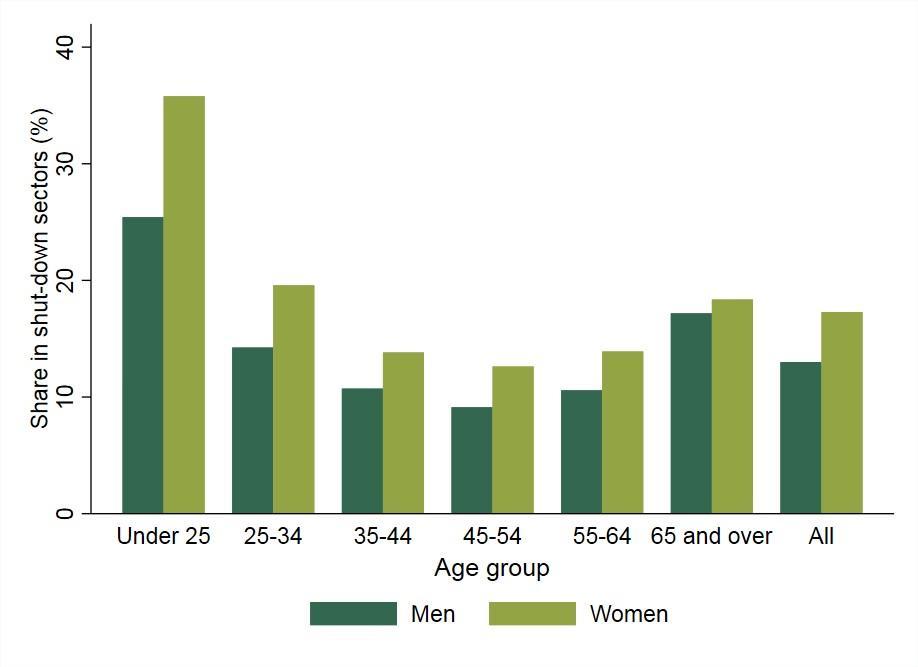
Figure 5
Source: This graph is reproduced from analysis by The Institute for Fiscal Studies on issues relating to home working and the labour market176. For a fuller description of the issues see https://www.ifs.org.uk/publications/14791
Different ethnic groups may also be differently affected by lockdown and remote schooling. Pakistani and Bangladeshi families (and to a lesser extent Indian and Black African families) are more likely to have an economically inactive woman in a household, meaning they may be better able to provide childcare and support home schooling with little impact on other adults in the household who are doing paid work and hence minimal impact on household income177178. However, most minority ethnic groups are also more likely to work in shut down sectors, and some groups have a higher probability of being self-employed179. The self-employed have seen large falls in income during the pandemic and are also more likely to be lower income in the first place. Hence the negative impact of the pandemic for many minority ethnic groups is more likely to be via a reduction in their household income rather than the direct impact of school closures on parents’ ability to work.
b. What we need to do
Evidence documenting the impact of school closures and social distancing on children’s mental health and other outcomes is accumulating, though much of it at this stage is self-report survey data. Again, it is important to note the urgency of good data and research on these issues since this level of isolation is unprecedented180. Care is needed since many of the early surveys of children’s experiences during the pandemic were not random samples and hence not representative of the population. A priority is longitudinal high-quality mental and physical health data on children and adolescents over the short and medium term to adequately monitor the impact of this pandemic181.
That said, a number of high-quality open access data sources are indeed coming on line, including follow up surveys of a number of ESRC funded large scale national longitudinal studies. The list below is not comprehensive but gives some sense of the scale of data that will be available within the next few months:
-
Understanding Society182. This is the large-scale UK Household Longitudinal Study, based at the Institute for Social and Economic Research (ISER) at the University of Essex. Understanding Society (US) went into the field in April 2020. 17,450 participants completed the survey in the first Wave. The 20-minute survey asked parents a range of questions about the impact of COVID-19. It had a particular focus on the impact of home schooling. It collected data on adult mental health but not child mental health (minimum age of respondent was age 16).
-
The Centre for Longitudinal Studies (CLS) launched a COVID related survey across 5 of its cohorts in May 2020, asking similar questions of 50,000 respondents. Questions covered physical and mental health, schooling and social contact. A number of the studies include respondents with children. The relevant studies for data on impacts on children are:
a. Millennium Cohort Study (born 2000-02)
b. Next Steps (born 1989-90)
c. 1970 British Cohort Study.
-
The Avon Study of Parents and Children have collected data from their cohorts which consist of a parent cohort (n=3720 mean age 59) and a “child” or second-generation cohort (n=2850 mean age 28). Since these are longitudinal surveys, comparison with pre COVID measures are possible. Survey questions included standard measures of depression and anxiety. Obviously this study cannot inform us about mental health in children given the age of the cohorts but it is worth noting that they found increases in anxiety and reductions in wellbeing particularly in younger populations, women, low income households and those with pre-existing health conditions183.
-
The National Study of Health and Wellbeing: Children and Young people is planning a 2020 follow up of the parents, children and adolescents who took part in the previous 2017 survey. The latter was a representative sample for England. The focus of the follow up survey will be on documenting mental health, physical health, development and emotional disorders, and comparing pre COVID measures with data collected during the pandemic.
-
The UK Household Longitudinal Study administered a web based survey which was completed by 17,452 panel members in April 2020. This survey assessed panel members’ mental health using the 12-item General Health Questionnaire. Initial analysis suggests that young people, women and those living with young children saw the greatest deterioration in mental health184.
-
ESRC has funded a University of Cardiff project led by Stephanie van Goozen to measure the impact of the pandemic on 300 primary school children who prior to COVID-19 were deemed by schools to be “at risk”, i.e. who already had emotional, cognitive, developmental or social vulnerabilities. They will focus on the impact of the pandemic period on these children’s mental health.
-
The MRC Cognition and Brain Sciences Unit at the University of Cambridge has gone into the field to collect data on 200 primary school children for which they have pre COVID-19 baseline data. The study, Resilience in Education and Development (RED) will provide rich data on children’s mental health. The longitudinal follow up took place in June 2020 and the study is led by Duncan Astle.
It is too early for results from these studies but they are likely to yield higher quality data than some early “snapshot” data, given their longitudinal dimension and that they are more representative of the relevant population. These studies should provide a rich picture of children and young people’s mental and physical health during the pandemic, and some aspects of their home schooling. They will not be able to show the impact of school closures on children’s health per se since they do not have a causal design and during the period of data collection most schools remained physically closed for most children. We would also suggest that when designing a study to capture the learning loss associated with school closures (see section 4), schools should also be asked to measure student wellbeing.
5. Commentary on the Government’s school opening plan & next steps
We note the recent (2/7/20) Department for Education (DfE) guidance regarding school opening in September 2020185. Its recognition of the significant costs of school closures, as well as the need to minimise the risks from opening schools, is to be welcomed. Our report supports the DfE position that all children need to return to face to face schooling wherever possible and that keeping schools open should be prioritised. School attendance must indeed be compulsory for the majority of children (i.e. those who are not at particular risk from COVID-19) and decisions to open and shut schools must be made on objective criteria with closures minimised. As we state above, what is urgently needed are clear and well communicated criteria to guide school closures and re-openings. This will also help to address teacher, parent and carer concerns about pupils returning to school.
The DfE guidance provides a lot of specific information for schools on how they should open and operate, as well as what will be required in preparation for a potential return to remote teaching during any future school closures. No doubt this guidance will change as the situation changes and more evidence emerges as to the effectiveness of different strategies to minimise infection transmission. Clear, realistic and timely communication with school leaders and teachers is vital. It is a major challenge to change ways of working in schools, particularly in a fast-moving environment with rapidly changing guidance. This needs to be recognised and guidance kept as simple and stable as possible. Further, some of the changes that are required of schools will need additional resource (whether that be in terms of additional staffing or pieces of PPE and other kit). This too needs to be recognised and an adequate level of resource provided. The challenge of simultaneously adapting schools to the safety mitigation procedures required, alongside also ensuring that adequate provision will be available in the event of subsequent school closures, should not be underestimated.
The DfE guidance also proposes additional resource to support academic catch up for pupils who have fallen behind. This will be vitally important if we are to mitigate some of the increasing inequality in academic achievement that we are likely to see as a result of the pandemic. The DfE guidance that schools need to support children’s wellbeing when they return is also supported by our report. However, again additional resources will be required. We also recommend that the Government develops policies and provides additional resource to support those students who have experienced learning and other losses from school closures to ensure they are not disadvantaged over their lifetime. We need to mitigate the economic scarring that will result from educational deficits in particular. The Government also needs to consider long term options to support re-entry to educational opportunity later in life for those disadvantaged by COVID-19 now.
As discussed at length in previous sections, there is much we still do not know. Further surveillance and studies are needed to:
-
Determine the extent to which children of different ages transmit COVID-19, including undertaking school case studies to better understand transmission processes;
-
Understand the effectiveness of different interventions and strategies designed to reduce infection transmission in schools, including learning from strategies being adopted in other countries;
-
Measure the learning and other losses from school closures during the pandemic; identify successful school interventions to reverse the detrimental impact of school closures on learning loss and other outcomes;
-
To address (2) and (3) we need to encourage experimentation, better evaluation and good knowledge exchange mechanisms to share learning across the education system.
Technical Appendices
The following are materials prepared by individual members of DELVE as inputs into this report.
- SCH-TD1: International comparisons of school policies
Prepared for the DELVE Initiative by
- SCH-TD2: Statistical designs for studies seeking to understand COVID-19 transmission in schools
Prepared for the DELVE Initiative by
Appendix: Estimates of the socio-economic gaps in learning
Standardised estimates for gap change during school closures, sourced from Education Endowment Foundation study.
| Study_year | Country | n_student | Subject | Disadvantage Definition | Δ̂i (delta_gap) |
SE${\widehat{(\Delta}}_{i})$ (standard error) |
(shrunken estimates) |
| burkam_2004 | USA | 3664 | Other | SES1 | 0.049 | 0.011 | 0.043 |
| davies_2013 | Canada | 1376 | Reading | SES2 | 0.011 | 0.004 | 0.011 |
| dumont_2020/quinn_2016 | USA | 3630 | Reading | SES3 | -0.021 | 0.005 | -0.018 |
| dumont_2020/quinn_2016 | USA | 3630 | Maths | SES3 | -0.001 | 0.005 | 0.000 |
| dumont_2020/quinn_2016 | USA | 3750 | Reading | SES3 | 0.016 | 0.006 | 0.017 |
| dumont_2020/quinn_2016 | USA | 3740 | Maths | SES3 | 0.043 | 0.006 | 0.041 |
| lindahl_2001 | Sweden | 556 | Maths | SES4 | 0.009 | 0.024 | 0.017 |
| meyer_2017 | Germany | 51 | Other | Parental occupation5 | -0.019 | 0.057 | 0.018 |
| meyer_2017 | Germany | 51 | Reading | Parental occupation5 | 0.113 | 0.076 | 0.028 |
| paechter_2015 | Austria | 180 | Maths | Mother’s education6 | 0.073 | 0.013 | 0.059 |
| verachtert_2009 | Belgium | 829 | Maths | SES7 | 0.012 | 0.029 | 0.019 |
| vonhippel_2019 | USA | 17779 | Maths | FRPL status8 | 0.014 | 0.005 | 0.014 |
| vonhippel_2019 | USA | 17779 | Reading | FRPL status8 | 0.015 | 0.004 | 0.015 |
| vonhippel_2019 | USA | 790 | Reading | FRPL status8 | 0.033 | 0.014 | 0.030 |
| vonhippel_2019 | USA | 790 | Maths | FRPL status8 | 0.047 | 0.012 | 0.041 |
Study_year: first author, and the year in which the study was published; Country; n_students: number of students reported in the study; Subject: “Other” represents either the general knowledge test in the ECLS-K study, or writing tests; Disadvantage definition: 1 Composite measure of parents’ education, parents’ occupational prestige, and household income; 2 composite measure of parent education, other parent education, income each standardised and summed; 3 NCES-created socioeconomic status (SES) variable, which is a composite of family income, parental education, and occupational prestige; 4 Census-based measure, combining the mean income and mean parental years education on the block of the relevant student, among households on that block where parents are aged 28-54 and kids are aged 10-12; 5 Highest Socio-Economic Index of Occupational Status; 6 Binary indicator for whether or not a mother sat the university entrance exam; 7 Composite measure including the educational level of both parents, the professional status of both parents, and the household income; 8Free and Reduced Price Lunch status. Delta_gap [Δ]: main outcome variable defined as the rate of change in the gap between FSM6 and nonFSM6 pupils, measured in effect-size units per month. SE_Delta_gap: (SE(Δ)): standard error of Δ
Source: Education Endowment Foundation (2020). Impact of school closures on the attainment gap: Rapid Evidence Assessment. London: Education Endowment Foundation, Table 2. Available at: https://educationendowmentfoundation.org.uk/public/files/EEF_(2020)_-_Impact_of_School_Closures_on_the_Attainment_Gap.pdf
Acknowledgements
In addition to those participating in the DELVE Initiative, the following provided input that helped inform this report: Evropi Theodoratou, Xue Li, Wei Xu, Marshall Dozier, Yazhou He, Amir Kirolos, Zhongyu Lang, William Browne, Mike Campbell, Nick Latimer, Sukriti Verma, Robbie Coleman, Carole Willis, Caroline Sharp, Monica Costa Dias, Harry Campbell, Ruth McQuilian, Harish Nair, Emilie McSwiggan, Gerry Fowkes; Halima Abiola, Gareth Andrews, Sarah Haythornthwaite, Rob Benzies, CUSP (Cambridge University Cross-Disciplinary Special Interest Group for Policy related to children and young people), Osama Rahman, Gary Lewis, Jonathan Simons, Stephen Sparks, Russell Viner, and two anonymous school leaders.
Footnotes and References
-
GOV.UK (2020) Education plans from September 2020. Available at https://www.gov.uk/guidance/education-plans-from-september-2020 [Accessed 9th July 2020]. ↩
-
There are a range of other education related issues arising from this pandemic, such as its impact on students’ progression to university, the loss of apprenticeships or the impact of the economic crisis on the graduate unemployment rate. However, in this report we focus exclusively on the issue of school closures. ↩
-
WHO, UNICEF & IFRC (2020) Key Messages and Actions for COVID-19 Prevention and Control in Schools. Available at: https://www.who.int/docs/default-source/coronaviruse/key-messages-and-actions-for-COVID-19-prevention-and-control-in-schools-march-2020.pdf?sfvrsn=baf81d52_4&download=true [Accessed 2 July 2020]. ↩
-
WHO (2020) Considerations for school-related public health measures in the context of COVID-19. Available at: https://www.who.int/publications/i/item/considerations-for-school-related-public-health-measures-in-the-context-of-covid-19 [Accessed 1st July 2020]. ↩
-
UNICEF, the World Bank, the World Food Programme and UNHCR (2020) Framework for reopening schools. Available at: https://www.unicef.org/sites/default/files/2020-06/Framework-for-reopening-schools-2020.pdf [Accessed 2 July 2020]. ↩
-
Office for National Statistics (2020) Coronavirus (COVID-19) infections in the community in England: July 2020. Characteristics of people testing positive for the coronavirus (COVID-19) in England from the COVID-19 Infection Survey. 7 July 2020. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronavirusCOVID19infectionsinthecommunityinengland/july2020. ↩
-
Pollán, M. et al (2020) Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. The Lancet, to appear. doi: 10.1016/S0140-6736(20)31483-5. ↩
-
Lavezzo, E. et al. (2020) Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vò, Nature (2020), to appear. doi: 10.1038/s41586-020-2488-1 ↩
-
Gudbjartsson, D.F. et al. (2020) Spread of SARS-CoV-2 in the Icelandic Population, N. Engl. J. Med. 382 (2020), pp. 2302-2315.doi: 10.1056/NEJMoa2006100 ↩
-
Public Health Agency of Sweden (2020) Initial results from ongoing investigation of antibodies to COVID-19 virus, 20 May 2020.Available at: https://www.folkhalsomyndigheten.se/nyheter-och-press/nyhetsarkiv/2020/maj/forsta-resultaten-fran-pagaende-undersokning-av-antikroppar-for-COVID-19-virus/ ↩
-
Birrell, P. et al. (2020) COVID-19: Nowcast and Forecast, 13 July
- Available at: https://www.mrc-bsu.cam.ac.uk/now-casting/
-
Centre for Disease Control and Prevention (2019) Estimated influenza illnesses, medical visits, hospitalizations and deaths in the United States, 2018-19 influenza season. Available at: https://www.cdc.gov/flu/about/burden/2018-2019.html. ↩
-
Birrell, P. et al. (2020) COVID-19: Nowcast and Forecast, 13th July 2020. Available at: https://www.mrc-bsu.cam.ac.uk/now-casting/ ↩
-
Ferguson, N. et al. (2020) Report 9: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. Imperial College COVID-19 Response Team, 16th March 2020. doi: 10.25561/77482. ↩
-
The Kids Corona Platform, SJD Barcelona Children’s Hospital. Further information available at: https://www.sjdhospitalbarcelona.org/en/kidscorona ↩
-
Royal College of Paediatrics and Child Health (2020) PIMS: the COVID-19 linked syndrome affecting children – information for families. Available at: https://www.rcpch.ac.uk/resources/pims-COVID-19-linked-syndrome-affecting-children-information-families. ↩
-
Davies, P. et al. (2020) Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. The Lancet, to appear. doi: 10.1016/S2352-4642(20)30215-7 ↩
-
Paediatric Intensive Care Audit Network (2019) Annual Report
- Available at:
https://www.picanet.org.uk/wp-content/uploads/sites/25/2019/12/PICANet-2019-Annual-Report-Summary_v1.0.pdf ↩
-
# Li, W. et al. (2020) Characteristics of Household Transmission of COVID-19. Clin. Infec. Dis. ciaa450, doi: 10.1093/cid/ciaa450. ↩
-
Jing, Q-L. et al. (2020) Household secondary attack rate of COVID-19 and associated determinants in Guangzhou, China: a retrospective cohort study. Lancet Infec. Dis., to appear. doi: 10.1016/S1473-3099(20)30471-0. ↩ ↩2
-
Mizumoto, K. et al (2020) Age specificity of cases and attack rate of novel coronavirus disease (COVID-19). medRxiv preprint. doi: 10.1101/2020.03.09.20033142. ↩
-
Zhang, J. et al. (2020) Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China, Science 368 (2020), 1481-1486. doi: 10.1126/science.abb8001 ↩
-
Bi, Q. et al. (2020) Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzen, China: a retrospective cohort study. Lancet Infec. Dis. 2020, to appear. doi: 10.1016/S1473-3099(20)30287-5. ↩
-
Boast, A. et al. (2020) An evidence summary of paediatric COVID-19 literature, Don’t Forget the Bubbles, 2020. Available at http://doi.org/10.31440/DFTB.24063. ↩
-
Hayward, AC. et al. (2014) Comparative community burden and severity of seasonal and pandemic influenza: results of the Flu Watch cohort study. The Lancet Respiratory Medicine 2 (2014), 445-454. doi: 10.1016/S2213-2600(14)70034-7 ↩
-
Baguelin, M. et al. (2013) Assessing optimal target populations for influenza vaccination programmes: an evidence synthesis and modelling study. PLoS Med. 10, 1-19. doi: 10.1371/journal.pmed.1001527 ↩
-
New South Wales Government and National Centre for Immunization and Surveillance (2020) COVID-19 in schools – the experience in NSW. Published 26 April 2020. Available at: http://ncirs.org.au/sites/default/files/2020-04/NCIRS%20NSW%20Schools%20COVID_Summary_FINAL%20public_26%20April%202020.pdf ↩
-
Yung, C.F. et al (2020) Novel Coronavirus 2019 Transmission Risk in Educational Settings. Clin. Infec. Dis. ciaa794. doi: 10.1093/cid/ciaa794. ↩
-
Heavey, L. et al. (2002) No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020. Eurosurveillance 25 (2002). doi: 10.2807/1560-7917.ES.2020.25.21.2000903. ↩
-
Fontanet, A. et al (2020) Cluster of Covid-19 in Northern France: A retrospective closed cohort study. medRxiv preprint, 23 April 2020. doi: 10.1101/2020.04.18.20071134. ↩
-
Kadari-Ovadia, S. et al. (2020) Schools in Jerusalem shut as dozens of students, staff test positive for virus, Haaretz, 1st June 2020. Available at: https://www.haaretz.com/israel-news/.premium-half-of-new-coronavirus-cases-in-schools-came-from-single-school-in-jerusalem-1.8885755 ↩
-
Torres, JP. et al (2020) SARS-CoV-2 antibody prevalence in blood in a large school community subject to a Covid-19 outbreak: a cross-sectional study. Clin. Infect. Dis. ciaa955, doi: 10.1093/cid/ciaa955. ↩
-
A project, led by John Jerrim at UCL, is planned to undertake a comprehensive assessment of teachers’ health in England drawing on numerous national survey data sets, including UK Biobank and the OECD’s Teaching and Learning International Survey (TALIS). ↩
-
UK Government (2020) Ethnicity facts and figures. Available at: https://www.ethnicity-facts-figures.service.gov.uk/uk-population-by-ethnicity/demographics/families-and-households/latest#asian-ethnic-group-by-household-type. ↩
-
Office for National Statistics (2020) One in eight British households has no garden. Available at: https://www.ons.gov.uk/economy/environmentalaccounts/articles/oneineightbritishhouseholdshasnogarden/2020-05-14 ↩
-
Office for National Statistics (2020) Deaths involving COVID-19 by local area and socioeconomic deprivation: deaths occurring between 1 March and 31 May 2020. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingCOVID19bylocalareasanddeprivation/deathsoccurringbetween1marchand31may2020. ↩
-
Guan, W. et al. (2020) Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. European Respiratory Journal. 55(5): 2000547 doi: 10.1183/13993003.00547-2020 ↩
-
UK Government (2020) Ethnicity facts and figures. Available at: http:www.ethnicity-facts-figures.service.gov.uk/health/diet-and-exercise/overweight-adults/latest ↩
-
Yang, J. et al. (2020) Prevalence of comorbities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. International Journal of Infections Diseases. 94: 91-95. doi: 10.1016/j.ijid.2020.03.017 ↩
-
Goff, LM. (2019) Ethnicity and Type 2 diabetes in the UK. Diabetic Medicine. 36: 927-938 12 doi: 10.1111/dme.13895 ↩
-
Shekerdemian, L. et al. (2020) Characteristics and Outcomes of Children with Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. Jama Pediatric doi:10.1001/jamapediatrics.2020.1948 ↩
-
Nelson, A. (2002) Unequal treatment: confronting racial and ethnic disparities in health care. Journal of National Medical Association. 94(8): 666-668. doi: 10.17226/12875 ↩
-
Anderson, KO. et al. (2009) Racial and ethnic disparities in pain: Causes and consequences of unequal care. J Pain; 10(12):1187-1204. doi: 10.1016/j.jpain.2009.10.002 ↩
-
Bonham, VL.( 2001) Race, ethnicity and pain treatment: Striving to understand the causes and solutions to the disparities in pain treatment. J Law Med Ethics. 29(1):52-68 doi: 10.1111/j.1748-720X.2001.tb00039.x ↩
-
UK Government (2020) Ethnicity facts and figures. Available at: https://www.ethnicity-facts-figures.service.gov.uk/uk-population-by-ethnicity/demographics/families-and-households/latest#asian-ethnic-group-by-household-type. ↩
-
Siddiqi, A. et al. (2017) Associations between race, discrimination and risk for chronic disease in a population-based sample from Canada. Soc Sci Med,194:135-141. doi: 10.1016/j.socscimed.2017.10.009 ↩
-
Viner, R., Russell, S., Croker, H., Packer, J., Ward, J., Stansfield, C., Mytton, O. and Booy, R. (2020) School Closure and Management Practices During Coronavirus Outbreaks Including COVID-19: A Rapid Narrative Systematic Review. SSRN Electronic Journal, doi: 10.2139/ssrn.3556648. ↩
-
Jones, E., Young, A., Clevenger, K., Salimifard, P., Wu, E., Lahaie Luna, M., Lahvis, M., Lang, J., Bliss, M., Azimi, P., Cedeno-Laurent, J., Wilson, C., Allen, J. (2020) Healthy Schools: Risk Reduction Strategies for Reopening Schools. Harvard T.H. Chan School of Public Health Healthy Buildings program. Available at: https://schools.forhealth.org/wp-content/uploads/sites/19/2020/06/Harvard-Healthy-Buildings-Program-Schools-For-Health-Reopening-Covid19-June2020.pdf ↩
-
Clalit Health Services, (2020). חולי קורונה בישראל: תמונת מצב | שירותי בריאות כללית. Accessed July 19, 2020. Available at: https://www.clalit.co.il/he/your_health/family/Pages/corona_in_israel.aspx ↩
-
Our World in Data (2020) Data source available at https://ourworldindata.org/grapher/weekly-COVID-cases?tab=chart&country=DEU~NLD~GBR [Accessed 26 June 2020] ↩
-
Flaxman, S. et al. (2020) Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature(2020) doi: 10.1038/s41586-020-2405-7 ↩
-
Thelocal.de (2020) Schools in German district to close after 400 meat factory workers test positive for coronavirus. Available at: https://www.thelocal.de/20200617/schools-and-kitas-in-german-district-to-close-after-400-workers-at-meat-factory-test-positive-for-coronavirus [Accessed 23rd June 2020]. ↩
-
BBC News (2020) Germany not alarmed by infection rate rise. Available at: https://www.bbc.co.uk/news/world-europe-52632369 [Accessed May 12, 2020] ↩
-
BR24. (2020). Corona An Schulen: Quarantäne Für Fast 100 Menschen In Neu-Ulm. Available at: https://www.br.de/nachrichten/bayern/corona-an-schulen-quarantaene-fuer-fast-100-menschen-in-neu-ulm,S3K1Li1 [Accessed 19 July] ↩
-
ynetnews. (2020). Israel To Reopen Schools On September 1 With Major Virus Adjustments. Available at: https://www.ynetnews.com/article/ByTW6IXkw [Accessed 19 July 2020] ↩
-
DELVE Initiative (2020), Face Masks for the General Public. DELVE Report No. 1. Published 04 May 2020. Available from http://rs-delve.github.io/reports/2020/05/04/face-masks-for-the-general-public.html. ↩
-
Services.aap.org. (2020). COVID-19 Planning Considerations: Guidance For School Re-Entry. Available at: https://services.aap.org/en/pages/2019-novel-coronavirus-COVID-19-infections/clinical-guidance/COVID-19-planning-considerations-return-to-in-person-education-in-schools/ [Accessed 19 July 2020] ↩
-
Centers for Disease Control and Prevention. (2020). Communities, Schools, Workplaces, & Events. Availble from https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/schools.html [Accessed 19 July 2020] ↩
-
Lewkowicz, D. J. & Hansen-Tift, A. (2012). Infants deploy selective attention to the mouth of a talking face when learning speech. Proceedings of the National Academy of Sciences, USA, 109(5), 1431-1436. doi: 10.1073/pnas.1114783109 ↩
-
Barenholtz, E., Mavica, L., & Lewkowicz, D. J. (2016). Language familiarity modulates relative attention to the eyes and mouth of a talker. Cognition, 147, 100-105. doi: 10.1016/j.cognition.2015.11.013 ↩
-
Holgate, S. et al (2020) Preparing for a challenging winter, 2020/21. Academy of Medical Sciences, 14 July 2020. Available from: https://acmedsci.ac.uk/file-download/51353957. ↩
-
Cunha, F. and Heckman, J.J. (2008). Formulating, identifying and estimating the technology of cognitive and noncognitive skill formation. Journal of human resources, 43(4), pp.738-782. ↩
-
Carlsson, M., Dahl, G. B., Öckert, B. and Rooth, D. (2015) The Effect of Schooling on Cognitive Skills. Review of Economics and Statistics vol. 97(3) pp. 533–547. ↩
-
Lavy. V. (2015) Do Differences in Schools’ Instruction Time Explain International Achievement Gaps? Evidence from Developed and Developing Countries. Economic Journal vol 125, ↩
-
Burgess, S. and Sievertsen H.H (2020) Schools, skills, and learning: The impact of COVID-19 on education. The Centre for Economic Policy Research. Available at: https://voxeu.org/article/impact-COVID-19- education ↩
-
Goodman, J. (2014). Flaking out: Student absences and snow days as disruptions of instructional time (No. w20221). National Bureau of Economic Research. ↩
-
Aucejo, E.M. and Romano, T.F. (2016) Assessing the effect of school days and absences on test score performance. Economics of Education Review, 55, pp.70-87. ↩
-
Cattan, S., Kamhöfer, D., Karlsson, M. and Nilsson, T., 2017. The short-and long-term effects of student absence: evidence from Sweden. Institute of Labor Economics, IZA DP 10995. ↩
-
Sacerdote, B. (2012) When the Saints Go Marching Out: Long-Term Outcomes for Student Evacuees from Hurricanes Katrina and Rita. American Economic Journal: Applied Economics, 4(1):109-35. ↩
-
Hattie, J. (2020) Visible Learning Effect Sizes When Schools Are Closed: What Matters and What Does Not. mimeo. Availale at: https://opsoa.org/application/files/2215/8689/0389/Infuences-during-Corona-JH-article.pdf ↩
-
Beaglehole, B., Bell, C. Frampton, C, and Moor, St. (2017) The impact of the Canterbury earthquakes on successful school leaving for adolescents. Australian and New Zealand Journal of Public Health. Vol 41 (1) pp. 70-73. ↩
-
Cooper, H., Nye, B., Charlton, K., Lindsay, J., & Greathouse, S. (1996). The Effects of Summer Vacation on Achievement Test Scores: A Narrative and Meta-Analytic Review. Review of Educational Research, 66(3), 227–268. doi: 10.3102/00346543066003227 ↩
-
von Hippel, P. T. and Hamrock, C. (2019). Do test score gaps grow before, during, or between the school years? Measurement artifacts and what we can know in spite of them. Sociological Science, 6, 43-80 ↩
-
# See von Hippel, P. T. (2019) Summer Learning: Key Findings Fail to Replicate, but Programs Still Have Promise. Education Next, https://www.educationnext.org/summer-learning-key-findings-fail-replicate-but-programs-still-promise/ and Von Hippel, P. T. (2019) Is Summer Learning Loss Real? Education Next. Vol 19, no. 4. https://www.educationnext.org/is-summer-learning-loss-real-how-i-lost-faith-education-research-results/ ↩
-
Atteberry, A. and McEachin, A. (2019). School’s Out: The Role of Summers in Understanding Achievement Disparities. (EdWorkingPaper: 19-82). Retrieved from Annenberg Institute at Brown University: doi: 10.26300/2mam-bp02 ↩
-
Portes, J, (2020) The lasting scars of the Covid-19 crisis: Channels and impacts. VOX-EU. Available at: https://voxeu.org/article/lasting -scars-COVID-19-crisis ↩
-
Jaume, D. and Willén, A. (2019) The Long-Run Effects of Teacher Strikes: Evidence from Argentina. Journal of Labor Economics vol. 37(4) pp. 1097 – 1139 ↩ ↩2
-
Office for National Statistics (2014) Intergenerational transmission of disadvantage in the UK & EU. Available at: http://webarchive.nationalarchives.gov.uk/20160105160709/http:/www.ons.gov.uk/ons/rel/household-income/intergenerational-transmission-of-poverty-in-the-uk---eu/2014/sty-causes-of-poverty-uk.html. Note that the ONS explicitly set this as the effect of education directly: “… the Individual’s assessment of their childhood household financial situation is not a significant predictor of poverty once educational attainment is accounted for.” ↩
-
Bennett, J., Pearson-Stuttard, J., Kontis, V., Capewell, S., Wolfe, I., and Ezzati, M. (2018) Contributions of diseases and injuries to widening life expectancy inequalities in England from 2001 to 2016: a population-based analysis of vital registration data. The Lancet Nov 22. doi: 10.1016/S2468-2667(18)30214-7 . ↩
-
Cattan, S., Conti, G., Farquharson, C. and Ginja, R., 2019. The health effects of Sure Start. Institute for Fiscal Studies. Available at: https://www.ifs.org.uk/publications/14139 ↩
-
Montacute, R. (2020) Social Mobility and COVID-19. Sutton Trust Report https://www.suttontrust.com/wp-content/uploads/2020/04/COVID-19-and-Social-Mobility-1.pdf ↩
-
Burgess, S. and Vignoles A. (2020) The Covid-19 crisis and educational inequality. Campaign for Social Science. Available at: https://campaignforsocialscience.org.uk/news/the-COVID-19-crisis-and-educational-inequality/ ↩
-
Education Endowment Foundation (2020). Impact of school closures on the attainment gap: Rapid Evidence Assessment. London: Education Endowment Foundation. Available at: https://educationendowmentfoundation.org.uk/public/files/EEF_(2020)_-_Impact_of_School_Closures_on_the_Attainment_Gap.pdf ↩
-
von Hippel, P. and Hamrock, C. (2019) Do Test Score Gaps Grow Before, During, or Between the School Years? Measurement Artifacts and What We Can Know in Spite of Them. Sociological Science, 6, pp.43-80. Available at: https://sociologicalscience.com/articles-v6-3-43/ ↩
-
Meyer F., Meissel, K., & McNaughton, S. (2017). Patterns of literacy learning in German primary schools over the summer and the influence of home literacy practices. Journal of Research in Reading 40(3), pp.233-253. ↩
-
Lindahl, M. (2001). Summer Learning and the Effect of Schooling: Evidence from Sweden. IZA
Discussion Paper No. 262. Available at: https://www.iza.org/publications/dp/262/summer-learningand-the-effect-of-schooling-evidence-from-sweden. ↩
-
Dumont, H. and Ready, D. (2020). Do Schools Reduce or Exacerbate Inequality? How the Associations Between Student Achievement and Achievement Growth Influence Our Understanding of the Role of Schooling. American Educational Research Journal, 57(2), pp.728-774. ↩
-
Quinn D., Cooc, N., McIntyre, J. and Gomez, C. (2016). Seasonal dynamics of academic achievement inequality by socioeconomic status and race/ethnicity: Updating and extending past research with new national data. Educational Researcher, 45(8), pp.443-453. ↩
-
Department for Education (2019) Key Stage 4 Performance 2019. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/863815/2019_KS4_revised_text.pdf ↩
-
Strand, S. (2014) Ethnicity, gender, social class and achievement gaps at age 16: Intersectionality and ‘Getting it’ for the white working class. Research Papers in Education, 29(2), pp.131-171. ↩
-
Full Fact (2020) Black Caribbean pupils three times more likely to be excluded. Available at: https://fullfact.org/education/black-caribbean-pupils-three-times-more-likely-be-excluded/ Accessed [June 23, 2020]. ↩
-
Office of National Statistics (2020) Child poverty and education outcomes by ethnicity. Available at: https://www.ons.gov.uk/economy/nationalaccounts/uksectoraccounts/compendium/economicreview/february2020/childpovertyandeducationoutcomesbyethnicity. Accessed [June 23, 2020]. ↩
-
Gillborn, D., Demack, S., Rollock, N. and Warmington, P. (2017) Moving the goalposts: Education policy and 25 years of the Black/White achievement gap. British Educational Research Journal, 43(5), pp.848-874. ↩
-
Shand-Baptiste, K. (2020) UK Schools have targeted black children for generations-the education system is overdue for a reckoning. The Independent. https://www.independent.co.uk/voices/school-racism-black-students-exclusions-hair-kiss-teeth-a9280296.html ↩
-
Ethnicity Facts and Figures (2019) Destinations and earnings of graduates after higher education. Available at: https://www.ethnicity-facts-figures.service.gov.uk/education-skills-and-training/after-education/destinations-and-earnings-of-graduates-after-higher-education/latest#average-earnings-of-graduates-by-ethnicity. Accessed [June 22, 2020] ↩
-
Office of National Statistics (2020) Child poverty and education outcomes by ethnicity. Available at: https://www.ons.gov.uk/economy/nationalaccounts/uksectoraccounts/compendium/economicreview/february2020/childpovertyandeducationoutcomesbyethnicity. Accessed [June 23, 2020]. ↩
-
Sutton Trust (2020) Coronavirus and Social Mobility Impact Brief #1: School Shutdown. Available at: https://www.suttontrust.com/our-research/coronavirus-and-social-mobility-impact-brief/. ↩
-
Andrew, A., Cattan, S., Costa-Dias, M., Farquharson, C., Kraftman, L., Krutikova, S., Phimister, A. and Sevilla, A. (2020). Learning During the Lockdown: Real-Time Data on Children’s Experiences During Home Learning. IFS Briefing Note BN288. Available at: https://www.ifs.org.uk /uploads/BN288-Learning-during-the-lockdown-1.pdf ↩
-
National Foundation for Educational Research (2020). Pupil engagement in remote learning. Available at: https://www.nfer.ac.uk/media/4073/schools_responses_to_COVID_19_pupil_engagement_in_remote_learning.pdf ↩
-
The study was funded by the Nuffield Foundation and NFER. ↩
-
Julius, J. and Sims, D. (2020). Schools’ Response to Covid-19: Support for Vulnerable Pupils and the Children of Keyworkers. (Forthcoming). Lucas, M., Nelson, J. and Sims, D. (2020). Schools’ Responses to Covid-19: Pupil Engagement in Remote Learning. [online]. Available at: https://www.nfer.ac.uk/media/4073/schools_responses_to_COVID_19_pupil_engagement_in_remote_learning.pdf [19 June 2020]. ↩
-
Sharp, C., Sims, D and Rutt, S. (2020). School’s Responses to Covid-19: Returning Pupils to School [online]. Available at: https://www.nfer.ac.uk/media/4060/schools_responses_to_COVID_19_early_report_final.pdf [19 June, 2020]. ↩
-
See page 19, Education Endowment Foundation (2019) Remote Learning: Rapid Evidence Assessment. Available at: https://educationendowmentfoundation.org.uk/public/files/Publications/Covid-19_Resources/Remote_learning_evidence_review/Remote_Learning_Rapid_Evidence_Assessment.pdf ↩
-
Means, B., Toyama, Y., Murphy, R., & Baki, M. (2013). The effectiveness of online and blended learning: A meta-analysis of the empirical literature. Teachers College Record, 115(3), 1–47. Available at: https://psycnet.apa.org/record/2013-11078-005 ↩
-
Andrew, A., Cattan, S., Costa Dias, M., Farquharson, C., Kraftman, L., Krutikova, S., Phimister, A. and Sevilla, A. (2020) How are mothers and fathers balancing work and family under lockdown? IFS Briefing Note 290. Available at: https://www.ifs.org.uk/uploads/BN290-Mothers-and-fathers-balancing-work-and-life-under-lockdown.pdf ↩
-
NFER (2020) Returning Pupils to Schools. Available at: https://www.nfer.ac.uk/media/4060/schools_responses_to_COVID_19_early_report_final.pdf ↩
-
Andrew, A., Cattan, S., Costa-Dias, M., Farquharson, C., Kraftman, L., Krutikova, S., Phimister, A. and Sevilla, A.. (2020) Learning during the lockdown: real-time data on children’s experiences during home learning. https://dera.ioe.ac.uk/35632/1/BN288-Learning-during-the-lockdown-1.pdf ↩
-
Department for Education (2020) COVID-19 and attendance statistics https://www.gov.uk/government/publications/coronavirus-COVID-19-attendance-in-education-and-early-years-settings ↩
-
Economists analyse the formation of skills as a production process, with inputs and outputs (see Cunha, F. and Heckman, J. (2007) The technology of skill formation. American Economic Review 97, pp. 31–47; Cunha, F., Heckman, J. and Schennach, S. (2010) Estimating the Technology of Cognitive and Noncognitive Skill Formation. Econometrica vol. 78(3) pp. 883–931. ↩
-
For most pupils; the pupils of key workers were permitted to go to school, but attendance was very patchy and for those who did attend, it could not be classified as a normal learning experience. ↩
-
Although many secondary schools test their incoming year7 pupils to get a sense of their abilities. ↩
-
It may be that such tests are available from NFER: https://www.nfer.ac.uk/ ↩
-
New York Times (2020) Research shows students falling months behind. Available at: https://www.nytimes.com/2020/06/05/us/coronavirus-education-lost-learning.html?auth=login-email&login=email ↩
-
Economics Observatory (2020) What are the effects of coronavirus on the UK and US labour markets? Available at: https://www.coronavirusandtheeconomy.com/question/what-are-effects-coronavirus-uk-and-us-labour-markets ↩
-
Office for National Statistics (2020) Claimant Count and Vacancies Time Series. Availale at: https://www.ons.gov.uk/employmentandlabourmarket/peoplenotinwork/unemployment/datasets/claimantcountandvacanciesdataset ↩
-
Marmot, M., Allen, J., Goldblatt, P., Boyce, T., McNeish, D., Grady, M. and Geddes, I. (2010) The Marmot review: Fair society, healthy lives. Strategic review of health inequalities in England post-2010. London: The Marmot Review. ↩
-
Bennett, J.E., Pearson-Stuttard, J., Kontis, V., Capewell, S., Wolfe, I. and Ezzati, M. (2018) Contributions of diseases and injuries to widening life expectancy inequalities in England from 2001 to 2016: a population-based analysis of vital registration data. The Lancet Public Health, 3(12), pp.e586-e597. ↩
-
Cooper, K. and Stewart, K. (2017) Does money affect children’s outcomes? An update. Available at: http://eprints.lse.ac.uk/103494/ ↩
-
Stuckler, D., Basu, S., Suhrcke, M., Coutts, A. and McKee, M. (2009) The public health effect of economic crises and alternative policy responses in Europe: an empirical analysis. Lancet. 2009;374(9686):315-323. doi:10.1016/S0140-6736(09)61124-7 ↩
-
Leon, D.A. (2016) Recessions and mortality: subtle but informative effects. Lancet. doi: 10.1016/S0140-6736(16)31712-3 ↩
-
Schneider, W., Waldfogel, J. and Brooks-Gunn, J. (2017) The Great Recession and risk for child abuse and neglect. Children and youth services review, 72, pp.71-81. ↩
-
Wang, G., Zhang, Y., Zhao, J., Zhang, J. and Jiang, F. (2020) Mitigate the effects of home confinement on children during the COVID-19 outbreak. The Lancet, 395(10228), pp.945-947. doi: 10.1016/ S0140-6736(20)30547-X ↩
-
Loades, ME., Chatburn, E., Higson-Sweeney, N., et al. (2020) Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J Am Acad Child Adolesc Psychiatry. 2020. doi: 10.1016/j.jaac.2020.05.009 ↩
-
Brooks, SK., Webster, RK., Smith, LE. et al. (2020) The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020. doi: 10.1016/S0140-6736(20)30460-8 ↩
-
Reynolds, S., Shafran, R., Brigden, A. and Linney, C. (2020) Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19, J Am Acad Child Adolesc Psychiatry. 2020. doi: 10.1016/j.jaac.2020.05.009 ↩
-
Crawley, E., Loades, M., Feder, G., Logan, S., Redwood, S. and Macleod, J. (2020) Wider collateral damage to children in the UK because of the social distancing measures designed to reduce the impact of COVID-19 in adults. BMJ Paediatrics Open, 4(1). ↩
-
Gunnell, D., Appleby, L., Arensman, E., Hawton, K., John, A., Kapur, N., Khan, M., O’Connor, R.C., Pirkis, J., Caine, E.D. and Chan, L.F. (2020) Suicide risk and prevention during the COVID-19 pandemic. The Lancet Psychiatry, 7(6), pp.468-471. doi: 10.1016/S2215-0366(20)30171-1 ↩
-
von Hippel, P.T. and Workman, J. (2016) From kindergarten through second grade, US children’s obesity prevalence grows only during summer vacations. Obesity, 24(11), pp.2296-2300. doi: 10.1002/oby.21613 ↩
-
Franckle, R., Adler, R. and Davison, K. (2014) Peer reviewed: accelerated weight gain among children during summer versus school year and related racial/ethnic disparities: a systematic review. Preventing chronic disease, 11. doi: 10.5888/pcd11.130355 ↩
-
Brooks, S.K., Webster, R.K., Smith, L.E., Woodland, L., Wessely, S., Greenberg, N. and Rubin, G.J. (2020) The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The Lancet. doi: 10.1016/S0140-6736(20)30460-8 ↩
-
Loades, ME., Chatburn, E., Higson-Sweeney, N. et al. (2020) Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J Am Acad Child Adolesc Psychiatry. doi: 10.1016/j.jaac.2020.05.009 ↩
-
Goodenow, C. (1993). Classroom belonging among early adolescent students: Relationships to motivation and achievement. Journal of Early Adolescence, 13(1), 21-43. doi: 10.1177/0272431693013001002 ↩
-
Burke, J., and Dempsey, M. (2020). Covid-19 Practice in Primary Schools in Ireland Report. doi: 10.13140/RG.2.2.14091.03369 ↩
-
Deci, E. L., and Ryan, R. M. (2008). Facilitating optimal motivation and psychological well-being across life’s domains. Canadian Psychology, 49(1), 14-23. doi: 10.1037/0708-5591.49.1.14 ↩
-
Hawkley, L.C. and Cacioppo, J.T. (2010) Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Annals of behavioral medicine, 40(2), pp.218-227. doi: 10.1007/s12160-010-9210-8 ↩
-
Caspi, A., Harrington, H., Moffitt, T.E., Milne, B.J. and Poulton, R. (2006) Socially isolated children 20 years later: risk of cardiovascular disease. Archives of pediatrics & adolescent medicine, 160(8), pp.805-811. doi: 10.1001/archpedi.160.8.805 ↩
-
Orben, A., Tomova, L. and Blakemore, S.J., 2020. The effects of social deprivation on adolescent development and mental health. The Lancet Child & Adolescent Health. doi: 10.1016/S2352-4642(20)30186-3 ↩
-
Blakemore, S.J. and Mills, K.L. (2014) Is Adolescence a Sensitive Period for Sociocultural Processing? Annu. Rev. Psychol. 65, 187–207 (2014) doi: 10.1146/annurev-psych-010213-115202 ↩
-
Bould, H., Mars, B., Moran, P., Biddle, L., Gunnell, D. (2019) Rising suicide rates among adolescents in England and Wales. Lancet, 394: 116–7. doi: 10.1016/S0140-6736(19)31102-X ↩
-
McManus, S., Gunnell, D., Cooper, C. et al (2019) Prevalence of non-suicidal self-harm and service contact in England, 2000-14: repeated cross-sectional surveys of the general population. The Lancet Psychiatry, 6: 573–81. doi: 10.1016/S2215-0366(19)30188-9 ↩
-
Hawton, K., Saunders, KEA., O’Connor, RC. (2012) Self-harm and suicide in adolescents. The Lancet, 379: 2373–82. doi: 10.1016/S0140-6736(12)60322-5 ↩
-
The National Child Mortality Database (2020) Child Suicide Rates during the COVID-19 Pandemic in England: Real-time Surveillance. Available at: https://www.ncmd.info/wp-content/uploads/2020/07/REF253-2020-NCMD-Summary-Report-on-Child-Suicide-July-2020.pdf ↩
-
Deighton, J., Humphrey, N., Belsky, J., Boehnke, J., Vostanis, P., and Patalay, P. (2017) Longitudinal pathways between mental health difficulties and academic performance during middle childhood and early adolescence. The British Journal of Developmental Psychology, Early View. doi: 10.1111/bjdp.12218 ↩
-
Panayiotou, M., & Humphrey, N. (2017). Mental health difficulties and academic attainment: Evidence for gender-specific developmental cascades in middle childhood. Development and Psychopathology, Early View, 1–16. doi: 10.1017/S095457941700102X ↩
-
Sadler, K., Vizard, T., Ford, T., Marchesell, F., Pearce, N., Mandalia, D., Davis, J., Brodie, E., Forbes, N., Goodman, A. and Goodman, R. (2018) Mental health of children and young people in England, 2017. NHS Digital report. Available at: https://dera.ioe.ac.uk/32622/1/MHCYP%202017%20Summary.pdf ↩
-
Walsh, G., Purdy, N., Dunn, J., Jones, S., Harrris, J. and Ballentine, M. (May 2020) Home Schooling in Northern Ireland and during the COVID-19 Crisis. The experience of parents and carers. CREU, Stranmillis College, Belfast ↩
-
Sadler K, Vizard T, Ford T, et al. (2018) Mental health of children and young people in England: Summary of key findings. NHS Digital. Available at: https://dera.ioe.ac.uk/32622/1/MHCYP%202017%20Summary.pdf ↩
-
Pearcey, S., Shum, A., Waite, P., Patalay, P.,Creswell, C. (2020) Report 04: Changes in children and young people’s emotional and behavioural difficulties through lockdown. Oxford: CoSPACE study; 16 June 2020 2020. Available at: https://emergingminds.org.uk/wp-content/uploads/2020/06/CoSPACE-Report-4-June-2020.pdf ↩
-
Levita L (2020). Initial research findings on the impact of COVID-19 on the well-being of young people aged 13 to 24 in the UK. COVID-19 Psychological Research Consortium (C19PRC), University of Sheffield; 7 May 2020 2020. ↩
-
XenZone (2020) Week 14: How Covid-19 is Affecting the Mental Health of Young People in the BAME Community. Published 11 June 2020. Available at: https://xenzone.com/wp-content/uploads/2020/06/BAME_infographic_June-2020_WEB-v2.pdf ↩
-
Viner, R., Patalay, P., Nicholls, D. et al. (2020) You-COPE: Youth COVID Response Personal Experience : Tracking health and wellbeing amongst 16-24 year olds in the UK during and after the COVID-19 pandemic. London: University College London (UCL). ↩
-
Children’s Commissioner for England (2020) Angry, fed up, isolated: Coronavirus and children’s mental health. Available at: https://www.childrenscommissioner.gov.uk/2020/04/03/angry-fed-up-isolated-coronavirus-and-childrens-mental-health/. ↩
-
Emerging Minds (n.d.). Co-SPACE study. Further information available at: Co-SPACE Study News ↩
-
Ford, T., Vostanis, P., Meltzer, H., and Goodman, R. (2007). Psychiatric disorder among British children looked after by local authorities: comparison with children living in private households. The British Journal of Psychiatry, 190(4), 319-325. doi: 10.1192/bjp.bp.106.025023 ↩
-
Bressan, S., Gallo, E., Tirelli, F., Gregori, D. and Da Dalt, L. (2020) Lockdown: more domestic accidents than COVID-19 in children. Arch Dis Child. doi: 10.1136/archdischild-2020-319547 ↩
-
Bhopal, S., Buckland, A., McCone, R., Villis, AI., Owens, S. (2020) Who has been missed? Dramatic decrease in numbers of children seen for child protection assessments during the pandemic. Arch Dis Child. doi: 10.1136/archdischild-2020-319783 ↩
-
YoungMinds (2020). Coronavirus: Impact on young people with mental health needs. Further information available at: https://youngminds.org.uk/about-us/reports/coronavirus-impact-on-young-people-with-mental-health-needs/ ↩
-
NSPCC Learning (2020). What children are saying to Childline about coronavirus. Available at: https://learning.nspcc.org.uk/research-resources/2020/childline-briefing-coronavirus ↩
-
Munkhaugen, EK., Gjevik, E., HugoPripp, A., Sponheim, E., Diseth, TH. (2017). School refusal behaviour: Are children and adolescents with autism spectrum disorder at a higher risk? Research in Autism Spectrum Disorders. 41–42, 31-38. doi: 10.1016/j.rasd.2017.07.001 ↩
-
Ochi, M., Kawabe, K., Ochi, S., Miyama, T.,Horiuchi, F. and Ueno, SI. (2020). School Refusal and Bullying in Children with Autism Spectrum Disorder. Child and Adolescent Psychiatry Mental Health. 14:17. doi: 10.1186/s13034-020-00325-7 ↩
-
Crawley, E., Loades, M., Feder, G., Logan, S., Redwood, S. and Macleod, J. (2020) Wider collateral damage to children in the UK because of the social distancing measures designed to reduce the impact of COVID-19 in adults. BMJ Paediatrics Open, 4(1). doi: 10.1136/bmjpo-2020-000701 ↩
-
Department of Social and Health Care (2020) What the Coronvirus bill will do. Available at: https://www.gov.uk/government/publications/coronavirus-bill-what-it-will-do/what-the-coronavirus-bill-will-do ↩
-
YoungMinds (2020). Coronavirus: Impact on young people with mental health needs. Further information available at: https://youngminds.org.uk/about-us/reports/coronavirus-impact-on-young-people-with-mental-health-needs/ ↩
-
Power, M., Doherty, B., Pybus, K. and Pickett, K. (2020) How COVID-19 has exposed inequalities in the UK food system: The case of UK food and poverty. Emerald Open Res 2020, 2:11 doi: 10.35241/emeraldopenres.13539.2 ↩
-
The Food Foundation (2020) Vulnerability to food insecurity since the COVID-19 lockdown. Available at: https://foodfoundation.org.uk/wp-content/uploads/2020/04/Report_COVID19FoodInsecurity-final.pdf ↩
-
Economists have done numerous analyses for the Economics Observatory and for VOX EU / CEPR on these and related labour market issues arising from the pandemic. See also analysis of these issues from The Institute for Fiscal Studies. ↩
-
Costa Dias, M., Farquharson, C., Griffith, R., Joyce, R. and Levell, P. (2020) Getting people back into work: IFS Briefing Note BN286. Available at: https://www.ifs.org.uk/uploads/BN286-Getting-people-back-into-work-1.pdf ↩
-
Economics Observatory (2020) Who can work from home and how does it affect their productivity? Available at:
https://www.coronavirusandtheeconomy.com/question/who-can-work-home-and-how-does-it-affect-their-productivity ↩
-
Economics Observatory (2020) How will the response to coronavirus affect gender equality? Available at: https://www.coronavirusandtheeconomy.com/question/how-will-response-coronavirus-affect-gender-equality ↩
-
Joyce, R. and Xu, X. (2020) Sector shutdowns during the coronavirus crisis: which workers are most exposed? IFS Briefing Note BN278. Available at: https://www.ifs.org.uk/publications/14791 ↩
-
Alon, T., Doepke, M., Olmstead-Rumsey, J. and Tertilt, M. (2020) The Impact of Covid-19 on Gender Equality. NBER WP 26947. https://www.nber.org/papers/w26947.pdf ↩
-
Economics Observatory (2020) How will the response to coronavirus affect gender equality? Available at: https://www.coronavirusandtheeconomy.com/question/how-will-response-coronavirus-affect-gender-equality ↩
-
Sevilla, A. and Smith, S. (2020) Childcare during a global pandemic: Many women left juggling work and childcare, but men do their share when they are not working. VoxEU CEPR, 16 June 2020. Available at:
https://voxeu.org/article/COVID-19-and-childcare-men-doing-their-share-only-if-they-are-not-working ↩
-
Understanding Society (2020) Covid-19 survey briefing note. Available at: https://www.understandingsociety.ac.uk/sites/default/files/downloads/general/ukhls_briefingnote_COVID_health_final.pdf ↩
-
Costa Dias, M., Farquharson, C., Griffith, R., Joyce, R. and Levell, P. (2020) Getting people back into work: IFS Briefing Note BN286. Available at: https://www.ifs.org.uk/publications/14829 ↩
-
Platt, L. and Warwick, R. (2020) COVID‐19 and Ethnic Inequalities in England and Wales. Fiscal Studies. doi: 10.1111/1475-5890.12228 ↩
-
Economics Observatory (2020) How is coronavirus affecting inequalities across ethnic groups? Available at https://www.coronavirusandtheeconomy.com/question/how-crisis-affecting-inequalities-across-ethnic-groups ↩
-
Platt, L. and Warwick, R. (2020) COVID‐19 and Ethnic Inequalities in England and Wales. Fiscal Studies. doi: 10.1111/1475-5890.12228 ↩
-
Holmes, E.A., O’Connor, R.C., Perry, V.H., Tracey, I., Wessely, S., Arseneault, L., Ballard, C., Christensen, H., Silver, R.C., Everall, I. and Ford, T. (2020) Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet Psychiatry. doi: 10.1016/S2215-0366(20)30168-1 ↩
-
Pierce, M., McManus, S., Jessop, C., John, A., Hotopf, M., Ford, T., Hatch, S., Wessely, S., Abel, K. (2020). A critical look at mental health surveys during COVID-19. The Lancet Psychiatry. doi: 10.17863/CAM.54251 ↩
-
Understanding Society (2020) Covid-19 Survey Briefing Note – home schooling. Available at: https://www.understandingsociety.ac.uk/sites/default/files/downloads/general/ukhls_briefingnote_COVID_homeschool_final.pdf ↩
-
Kwong, A.S.F., Pearson, R.M., Adams, M.J., Northstone, K., Tilling, K., Smith, D., Fawns-Ritchie, C., Bould, H., Warne, N., Zammit, S. and Gunnell, D.J. (2020) Mental health during the COVID-19 pandemic in two longitudinal UK population cohorts. medRxiv. doi: 10.1101/2020.06.16.20133116 ↩
-
Pierce, M., Hope, H., Ford, T., Hatch, S., Hotopf, M., Kontopantelis, E., John, A., Webb, R.T., Wessely, S., McManus, S. and Abel, K.M. (2020) Mental Health Before and During the COVID-19 Pandemic: A Longitudinal Probability Sample Survey of the UK Population. SSRN 3624264. doi: 10.1016/S2215-0366(20)30308-4 ↩
-
UK Government (2020) Education plans from September 2020 Available at https://www.gov.uk/guidance/education-plans-from-september-2020 [Accessed 9 July 2020]. ↩